Case Report

Caecal Epidermoid Cyst in an otherwise Healthy Young Man: A Case Report and Review of Literature.
1Houssam Abtar, 2 Johnny Haddad, 2Charbel Aoun,,3Tarek Mhana, 2Haytham Mochairefam
- 1.Makassed General Hospital, Department of Surgery, Beirut, Lebanon
- 2.Central Military Hospital, Department of Surgery, Beirut, Lebanon
- 3.Central Military Hospital, Department of Radiology, Beirut, Lebanon
- Submitted January 2, 2019;
- Accepted June 20, 2019;
- Published Saturday, July 6,2019
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction:
Epidermoid cysts of the abdominal organs (spleen, liver, and kidney) are known pathologies. Two varieties of epidermoid cyst are described, acquired and congenital. These lesions are diagnosed all the time after pathological evaluation.
Case Presentation:
Hereby, we report a case of a 23-year-old man, with an unremarkable previous medical history, who presented for chronic vague lower abdominal pain of several weeks duration associated with generalized fatigue and a non-significant weight loss. On physical exam a palpable right lower quadrant mass was noted which turned to be caecal epidermoid cyst on final pathology after surgical excision.
Conclusion:
Caecal epidermoid cyst is an extremely rare entity with only few reported cases have been described in the literature. On radiological imaging (computed tomography, magnetic resonance imaging) these lesions look like a cystic mass and can be mistaken as mesenteric cyst, cystic lymphangioma or gastro intestinal stromal tumor.
Keywords:
Caecum, epidermoid cyst, hemicolectomy
Introduction
Epidermoid cysts are lined by well differentiated stratified squamous epithelium and these cysts enlarge by cellular proliferation and desquamation of keratinized debris into the cyst center [1].Epidermoid cysts also called sequestration cysts, are believed to have congenital or acquired origin. Congenital epidermoid cysts are usually occurring in the head, neck and ano-rectum. They are mostly seen in patients without previous abdominal trauma or intra-abdominal surgery and probably resulted from aberrant implantation of ectodermal elements during embryogenesis. However, Acquired epidermoid cysts are traumatic or iatrogenic in nature [2].Epidermoid cysts of the abdominal organs are very rare with only limited cases have been reported in the testes, epididymis, spleen, liver and kidney [3].Caecal epidermoid cyst may have been originated during intrauterine rotation where the cecum re-enters the abdominal cavity as the last part of the gut [2].
Case Presentation
Herein, we present a case of 23 years old man, nonsmoker, well-being, with past surgical history significant only for right inguinal hernia repair performed 2 years prior to presentation. Patient was complaining of chronic, vague, lower abdominal pain, associated with generalized fatigue, constipation, and mild intermittent nausea. He denies fever or urinary symptoms.
He had an unremarkable overall physical exam. However, a visible right inguinal scar was noted; no visible abdominal wall hernias or organomegaly. A palpable mobile mass was noted in the right lower quadrant (RLQ) with mild overlying tenderness. Routine labs were requested and were reported as normal. (Hb: 16.6, Hct: 47.8, white count: 8100, platelet count: 160,000. Normal electrolyte panel as well as liver enzymes.)
A computed tomography (CT) Scan of the abdomen with intravenous contrast was ordered. A deep pelvic intraperitoneal cystic lesion about 6.5x5.5 cm is noted in the RLQ, abutting the urinary bladder superiorly without involvement of the major vessels (Figures 1). No lymphadenopathy, or other visible masses were recorded.
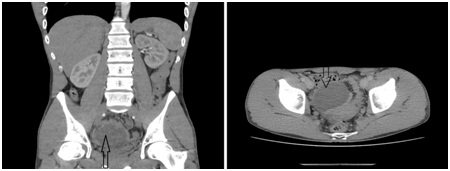
Figure 1: A computed tomography scan of the abdomen and pelvis showing a huge exophytic, 6.5x5.5 cm intrapelvic mass, abutting the urinary bladder (black arrow).
The differential diagnosis made by the radiologist was cystic lymphangioma, mesenteric or hydatid cyst. For better evaluation,a magnetic resonance imaging (MRI) with gadolinium of the abdomen and pelvis was done and reported as presence of a right sided pelvic cavity mass around 5.5 x 5.8 x 6.4 cm of hypersignal on T2 (white), hyposignal on T1 (black), without enhancement post gadolinium injection, suggestive of a probable mesenteric cyst (Figures 2).

Figure 2: MRI of the abdomen and pelvis with gadolinium revealed right sided pelvic cavity mass of hypersignal on T2, hyposignal on T1, without enhancement (white arrow).
At Exploratory laparotomy a round, soft, cheesy like mass with a thin membrane was noted with close proximity of the caecal wall, on the medial aspect, adjacent to the ileocecal valve (Figure 3). It was well circumscribed, had a smooth surface without cleavage plane between it and the caecum.

Figure 3: Intraoperative view of a round, soft, thin membrane mass arising from the caecum (white arrow).
An en-block resection of the mass along with the appendix and terminal ileum performed through right hemicolectomy (Figure 4). Patient had a smooth post-operative course and discharged home on day 5 post operation. The final pathological examination was reported as epidermoid cyst extending from the serosal surface of the caecum without any connection to the caecal lumen and appendix. No evidence of malignancy, negative surgical margins, and multiple reactive lymph nodes.

Figure 4: Surgical specimen after right hemicolectomy, showing subserosal lesion filled with cheesy material (black circle), along with the appendix (black arrow).
Discussion
Caecal epidermoid cysts are neither true neoplasms nor inflammatory in nature [4] Congenital cysts are linked to ectodermal implantation during closure of neural groove that occurs between 3rd and 5th week of embryonic life or coalescence of other epithelial fusion lines[1, 2].Epidermoid cysts have been reported in several internal organs including the testis, epididymis, spleen and liver [5, 6]. However, cysts of the cecum are extremely rare with only nine cases reported previously in the literature [Table 1].
Table 1: Reported cases of epidermoid cyst of the cecum in the literature.
Untitled 1
| Case number |
Age |
Sex |
History of operation |
Initial Diagnosis |
Location of epidermoid cyst |
Year reported |
| 1 |
22 |
Female |
Appendectomy(12 yrs. Before) |
Right lower abdominal mass |
Intramural |
1961 |
| 2 |
27 |
Female |
None |
Chronic appendicitis?
Ovarian cyst torsion?
|
Subserosal |
1965 |
| 3 |
71 |
Male |
Appendectomy(16 yrs. Before) |
Extrinsic, or intramural cecal mass |
Intramural |
1969 |
| 4 |
8 |
Female |
None |
Right lower abdominal cyst |
Subserosal |
1999 |
| 5 |
67 |
Male |
None |
Duplication cyst? |
Subserosal |
2002 |
| 6 |
75 |
Male |
None |
Appendix mucocele? |
Subserosal |
2006 |
| 7 |
31 |
Female |
Cesarean section |
Adnexal mass |
Subserosal |
2012 |
| 8 |
54 |
Male |
None |
Mesenteric cyst |
Subserosal |
2013 |
| 9 |
63 |
Female |
None |
GIST |
Intramural |
2015 |
| 10 |
23 |
Male |
Right inguinal hernia repair |
Mesenteric cyst |
Subserosal |
Our case |
History of abdominal surgery was seen in three of the reported cases, with two of them had history of appendectomy and the third cesarean section. The concept of iatrogenic implantation of epidermal fragments was adopted in these cases using surgical tools like scalpel, needle or clamp. The other cases had no history of abdominal surgeries, therefore adopting the concept of congenital cysts[2,7].
Andiran et al. stated that later development of the cysts can be caused by any inclusion or closure line of epidermal or dermal structures [4]. Moreover, this concept is supported by the fact that occurrence of the epidermoid cyst in a subserosal location in the cecum is seen in most of the cases including ours.
Epidermoid cysts of the cecum are subserosal lesions, for this reason the differential diagnosis of an epidermoid cyst is rarely considered before surgical resection [2, 3].On CT imaging, these cysts may be confused with other intra-abdominal cystic lesions, including mesenteric cysts, lymphatic cysts, appendiceal mucoceles or duplication cysts. In female patients, with initial diagnosis of right adnexal mass or cyst, ovarian cyst or a caecal epidermoid cyst must be considered [7]. Also, dermoid cysts should be kept in mind and they are differentiated from epidermoid cysts by their mature, squamous, epithelial cells lining and specialized skin structures, such as sweat glands, hair follicles, and sebaceous glands [1].
Diagnostic laparoscopy is minimally invasive surgery used for the diagnosis of intra-abdominal diseases which offers in future a potential significant role for diagnosis and management of epidermoid cysts [8]. It was utilized in one of the reported cases of caecal epidermoid cyst [3]. Iwasaki et al. [9] had a pre-diagnosis of mucinous cystic neoplasm of the pancreas undergone laparoscopic distal pancreatectomy. However, postoperative pathologic examination showed an epidermoid cyst arising from a heterotopic spleen within the pancreas. There was no need for conversion to open. Nevertheless, many studies have discussed the possibility of dissemination following laparoscopy including trocar site and intra-abdominal recurrence [10]. With these risks kept in mind, we had undergone exploratory laparotomy in our case.
Conclusion
Caecal epidermoid cyst remains an extremely rare pathology with a few reported cases in the literature, for this reason they rarely included in the differential diagnosis of caecal masses. They are subserosal lesions and can be confused with mesenteric or lymphatic cysts, mucoceles or gastro intestinal stromal tumor. Open or laparoscopic right hemicolectomy remains the procedure of choice for caecal epidermoid cyst.
Learning Points
-Epidermoidcysts of the cecum still represent an extremely rare entity with only nine cases reported previously in the literature.
-Diagnosis of a caecal epidermoid cyst before pathological evaluation remains a dilemma because of wide range of differential diagnosis.
-Right hemicolectomy by open or laparoscopic approach is the standard of care with no other treatment modalities is needed.
Consent of Patient
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Conflict of interest
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
Authors' Contributions
All authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript.
Houssam Abtar, CharbelAoun, Haytham Mochairefa: participated in patient’s surgery, outcomes and follow-up. Conception, design, writing and composition of the manuscript was also taken care of along with the critical revision of the article.
Johnny haddad: Responsible for patient’s investigation, diagnosis, clinical and treatment judgment by multidisciplinary evaluation, interpretation as well as critical revision of the article. He was also responsible for approving the final version to be published.
Tarek Mhana: Important contributions to the conception and design of the manuscript. Final correction and verification of scientific data of the article. He also approved the final version to be published.
Acknowledgements
None
References
[1].Pear BL. Epidermoid and dermoid sequestration cysts. Am J Roentgenol Radium TherNucl Med 1970; 110:148-55.[[PubMed]
[2].Park JY, Kim YW, Lee KY, Sung JY. Epidermoid Cyst of the Cecum. Ann Coloproctol. 2015 Feb;31(1):37-39.[Pubmed] [PMC Full text]
[3].Sahoo MR, Gowda MS, Behera SS. Unusual site and uncommon presentation of epidermoid cyst: a rare case report and review of literature. BMJ Case Rep. 2013 Jan 8;2013.[pubMed] [PMC Full text]
[4].Andiran F, Dayi S, Caydere M, Dilmen G, Dilmen U .Epidermoid cyst of the cecum. J Pediatr Surg. 1999 Oct; 34(10):1567-9.[Pubmed]
[5].Price EB Jr. Epidermoid cysts of the testis: a clinical and pathologic analysis of 69 cases from the testicular tumor registry. J Urol. 1969 Dec; 102(6):708-13. [PubMed]
[6].Schullinger JN, Wigger HJ, Price JB, Benson M, Harris RC. Epidermoid cysts of the liver. J Pediatr Surg. 1983 Jun;18(3):240-2.[Pubmed]
[7].Demır H, Aydoğan B, Şahın H, Öcal P, Ilvan Ş. Epidermoid cyst of the cecum: a case report. Turk J Gastroenterol. 2012 Aug;23(4):406-9.[pubMed]
[8].Richardson WS, Stefanidis D, Chang L, Earle DB, Fanelli RD. The role of diagnostic laparoscopy for chronic abdominal conditions: an evidence-based review. SurgEndosc. 2009 Sep;23(9):2073-7.[PubMed][Free full text]
[9].Iwasaki Y, Tagaya N, Nakagawa A, Kita J, Imura J, Fujimori T,Kubota K. Laparoscopic resection of epidermoid cyst arising from an intrapancreatic accessory spleen: a case report with review of the literature.SurgLaparoscEndoscPercutan Tech. 2011 Oct;21(5):e275-9.[Pubmed]
[10].FisherJ.C.,Gurung B., Cowles R.A. Recurrence after laparoscopic excision of nonparasitic splenic cysts. J Pediatr Surg. 2008 Sep;43(9):1644-8.[Pubmed]

