Case Report

Laparoscopic Atypical Gastrectomy For Symptomatic Gastric Lipoma
*Arnaldo Machado, *André
Oliva, * Manuel Carvalho,*,
Rosa Félix, *Jorge Caravana
- * General Surgery Service, Hospital does Espírito Santo E.P.E. Address: Largo Senhor da Pobreza 7000, Évora, Portugal;
- Submitted: Tuesday, February 13, 2018;
- Accepted:Saturday, March 17, 2018;
- Published:Sunday, March 18, 2018
This is an Open Access article distributed under the terms of the Creative Commons Attribution License ((http://creativecommons.org/licenses/by/4.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction
Gastric lipoma is a rare benign gastric tumor, usually found incidentally. Although most gastric lipomas are asymptomatic, they can cause abdominal pain, gastrointestinal bleeding and obstruction.
Case Presentation
A 51-year-old male patient presented with complaints of epigastric pain and haematemesis. The endoscopy showed an ulcerated polypoid lesion in the anterior gastric wall, 4cm in diameter, endoscopically unresectable. The computed tomography scan revealed no other lesions and the endoscopic ultrasound suggested a lipoma of the gastric wall. Preoperatively the lesion was marked with china ink.
The patient underwent a laparoscopic atypical gastrectomy, and the histology showed a gastric lipoma.
Discussion
Despite its rarity, gastric lipoma should be diagnosed histologically. Symptomatic benign gastric lesions not amenable to endoscopic removal should be excised by surgery. Laparoscopic atypical gastrectomy is an effective, safe and minimally invasive technique.
Key words
Gastric Lipoma; Laparoscopy; Atypical Gastrectomy
Introduction
Lipomas are benign submucosal tumors composed of mature adipose tissue. They may occur anywhere in the gastrointestinal tract. The incidence of gastric lipoma is rare, with only about 220 cases described in the literature. [1, 2]
The first description of gastric lipoma is attributed to Cruveilhier (1842). [3] These tumors may be found at any site of the stomach, but are more commonly located in the gastric antrum (75%). Almost 90% of the cases have origin in the submucosa and the rest are intramural or subserosal. [4]Although most gastric lipomas are usually detected incidentally, they can cause severe symptons such as gastrointestinal bleeding, abdominal pain, obstruction and intussusception. [2, 3]
Case Presentation
A 51-year-old man was admitted with a week duration history of epigastric pain associated with upper gastrointestinal bleeding. There was a previous intake of non-steroidal anti-inflammatory drugs for two weeks because of back pain. The patient had past medical history of obesity (IMC 32), diabetes mellitus and dyslipidaemia. There was no history of cigarette smoking, alcohol use, peptic ulcer disease, or reflux. His grandfather died at the age of 55 from gastric cancer. Laboratory tests showed low hemoglobin values (11 g/dL). The remaining blood cell count and chemistry profile were within normal limits.
He underwent an endoscopy study that disclosed an ulcerated polypoid lesion in the anterior gastric wall, with 4cm diameter endoscopically unresectable(Figure 1). The hemorrhage was treated by clipping and with adrenaline injection. The biopsy showed a chronic gastritis and the test for Helicobacter pylori was negative. Abdominal computed
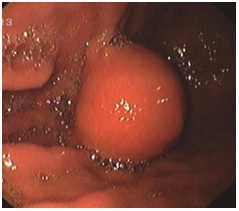
Figure 1 – Endoscopy show a polypoid lesion in the anterior gastric wall, with 4cm diameter endoscopically unresectable
tomography (CT) showed no apparent findings of secondary disease and the endoscopic ultrasound revealed mature fat tissue at the submucosa, suggesting a submucosal lipoma.
Preoperatively the lesion was marked through endoscopy with china ink (Figure 2A). The patient underwent a laparoscopic atypical gastrectomy (Figure 2A-D) to remove the gastric tumor with a wide free surgical margin. Three 12mm trocars (supraumbilical, right and left subcostal) and one 5mm (epigastric) were used. The tumor was removed using a laparoscopic collector bag through the umbilical port.
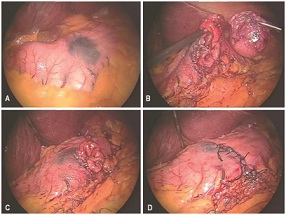
Figure 2 - Laparoscopic atypical gastrectomy to remove the gastric tumor (A-D), previously marked through endoscopy with
China ink (A).
The patient was discharged from the hospital asymptomatic and accepting solid foods on the 6th day after the procedure. No incidents were reported. Histology confirms that the polyp was a gastric lipoma (Figure 3A-B). Three years after surgery the patient is asymptomatic.
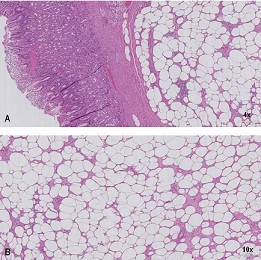

Figure 3 - Photomicrograph of the polyp A). showing the hypeprlastic gastric
mucosa overlying the fibrocollagenous tissue capping the superficial portion of
the lipoma (H&E ×4); B). The lipomatuos component composed of mature fat
cells intermixed with fibrocollagenous tissue (H&E ×10)
Discussion
Gastric lipomas are rare benign tumors, composed of a fibrous capsule surrounding mature adipose tissue. These account for 5% of all gastrointestinal lipomas and 3% of all benign tumors of the stomach. The etiology of gastric lipomas is unclear. It may be due to adipocytes embryological sequester, the natural process of aging or an acquired condition. [1, 5, 6] Gastric lipomas prevail between the fifth and seventh decades of life, with equal gender incidence. [3, 4]
They are usually small, asymptomatic and detected as incidental findings. In patients with larger lesions (> 3-4cm), severe symptons can be present. The most common complaints are hemorrhage, abdominal pain, dyspepsia and pyloric obstruction. [4, 5, 7, 8] Gastrointestinal bleeding is typically chronic and minimal but can lead to cause anemia.
Endoscopic findings of gastric lipomas are described as: “naked fat sign” (a yellowish colour), the “tenting” sign (easy retraction of the overlying mucosa with a biopsy forceps) and the “cushion” sign (impression after compressing the mass with the biopsy forceps). Biopsy is difficult and usually not diagnostic due to the submucosal nature of the lesion. It generally only reveals normal gastric mucosa. [3, 6]
Computed tomography has been shown to be valuable in the diagnosic workup. It demonstrated a well-circumscribed, submucosal mass with uniform fat density and attenuation, ranging between −70 and −120Hz. [2, 6]
Endoscopic ultrasound is useful for the diagnosis of gastric lipoma, it allows the identification of the tumor’s primary layer, and may reveal a possible invasion of the lymph nodes and peripheral layers. Typically, lipomas are visualized as hyperechoic homogeneous lesions that have regular margins and that arise from the third layer of the gastric wall. [6]
The most important differential diagnosis for gastric lipoma, aside from liposarcoma, is a gastrointestinal tract soft tissue tumor such as a gastrointestinal stromal tumor, leiomyoma, fibroma, and their malignant variables. [1, 2, 6]
Gastric lipomas have no malignant potential. However, synchronous gastric carcinomas have been very rarely described. These cases are believed to be coincidental. The presence of gastric submucosal tumors that extend into the gastric lumen may lead to erosions on the gastric epithelium or be themselves sites of inflamation, which are thought to be gastric cancer promoters. [9]
The treatment of gastric lipoma is still controversial. [1] Pedunculated lipomas, smaller than 3cm, may be excised by upper digestive endoscopy, although mere observation is a valid option. The reason for this is that malignant degeneration has not been reported. [4] For the majority of authors, surgical resection remains the treatment of choice for larger, symptomatic gastric lipoma. Laparoscopy is a minimally invasive surgery technique used for tumors up to 6 cm in diameter. [10, 11, 12, 13]
Conclusions
We report here a rare case of gastric lipoma coexisting with upper gastrointestinal bleeding. Resection is the best choice for symptomatic and endoscopically unresectable gastric lipomas. The indication for surgery in this patient was the gastrointestinal bleeding resulting in anaemia, recurring abdominal pain and the possibility of development of an outlet obstruction in the future, if not removed. Endoscopy is important to locate the tumor and laparoscopic atypical gastrectomy is an effective, safe and a minimally invasive surgery technique to treat this benign gastric tumor.
Learining points
Gastric lipoma is a rare benign gastric tumour generally asymptomatic.
Clinical presentation with upper gastrointestinal bleed is the commonest presenting symptom.
Surgery is reserved for symptomatic and endoscopically unresectable lipomas.
Laparoscopic gastric resection can be used for small lipomas.
Author’s contributions
All people who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript.
AM: responsible for patient’s follow-up; participation on patient’s surgery; conception, design and composition of the manuscript guided by the actual data and evidence; critical revision.
AO: Responsible for patient’s investigation, diagnosis, patient’s surgery, outcome and follow-up, data analysis, interpretation and also for doing the critical revision of the article; approved the final version to be published.
MC: Responsible for patient’s surgery, outcome and follow-up, data analysis, interpretation and also for doing the critical revision of the article; approved the final version to be published.
RF: Important contributions to the conception and design of the manuscript, drafting the article and doing critical revision; approved the final version to be published.
JC: Important part of clinical and treatment judgement by multidisciplinary evaluation, made critical revision of the article and approved the final version to be published.
Patient consent
A written consent was obtained from the patient.
Competing interests
The authors have no conflict of interests.
Acknowledgments
We thank Dr. Sara Pires for the endoscopy image and Dr.
Carlos Quintana for the collection of the lipoma histology images.
References
[1].Chagarlamudi K., Devita R.,& Barr R.G... Gastric Lipoma: A Review of the Literature. Ultrasound Q. 2018; 2018, Jan 23 [PubMed]
[2].Ramdass MJ, Mathur S, Seetahal-Maraj P, Barrow S. Gastric lipoma presenting with massive upper gastrointestinal bleeding. Case Rep Emerg Med. 2013; 506101. [PubMed]
[3].López-Zamudio J., Leonher-Ruezga K. L., Ramírez-González L. R., Razo Jiménez G., González-Ojeda A., & Fuentes-Orozco C.. Lipoma gástrico pediculado. Reporte de caso. Cir Cir. 2015; 83(3):222-6. [PubMed]
[Free
Full Text]
[4].Agrawal K., Soubam P. S., &Vaiphei K.. Two cases of rare benign mucosal lesions of the stomach. BMJ Case Rep. 2013; Jul 31;2013.[PubMed]
[PMC Full Text]
[5].Oh J. Y., Nam K. J., Choi J. C., Cho J. H., Yoon S. K., Choi S. S., et al. Benign submucosal lesions of the stomach and duodenum: Imaging characteristics with endoscopic and pathologic correlation. Eur J Radiol. 2008; 67(1), 112–124. [PubMed]
[6].Neto F.A., Ferreira M.C., Bertoncello L.C., Neto A.A., de Aveiro W.C., Bento C.A., et al. Gastric lipoma presenting as a giant bulging mass in an oligosymptomatic patient: a case report. J Med Case Rep. 2012; 6:317.[PubMed]
[PMC Full Text]
[7].Priyadarshi R.N., Anand U., Pandey M.K., Chaudhary B., Kumar R.. Giant Gastric Lipoma Presenting as Gastric Outlet Obstruction - A Case Report. J Clin Diagn Res. 2015 Oct 1.[PubMed][PMC
Full Text]
[8].\Almohsin M., & Meshikhes A.W.. Gastric lipoma presenting with haematemesis. BMJ Case Rep. 2015 Jan 29.[PubMed]
[PMC Full
Text]
[9].Yamamoto T., Imakiire K., Hashiguchi S., Matsumoto J., Kadono J., Hamada N.,, et al. A rare case of gastric lipoma with early gastric cancer. Intern Med. 2004 Nov;43(11):1039-41 [PubMed]
[Free
Full Text]
[10].Kim D.D., Tsai A.I., Otani A.R., Puglia C.R., Malheiros C.A... Gastric lipoma case report. Rev Col Bras Cir. 2011 May-Jun;38(3):205-6.[PubMed]
[Free
Full Text]
[11].Kang WM, Yu JC, Ma ZQ, Zhao Z.R., Meng Q.B., Ye X.. Laparoscopic-endoscopic cooperative surgery for gastric submucosal tumors. World J Gastroenterol. 2013 Sep 14; 19(34):5720-6.[PubMed]
[PMC Full Text]
[12].Olguín R R, Norero M E, Briceño E, Martínez C., Viñuela E., Báez S., et al. Gastric lipoma removed by laparoscopic subtotal gastrectomy: report of one case. Rev Med Chil. 2013 Jul; 141(7):927-31 [PubMed]
[Free
Full Text]
[13].Caron P.H., Martins M.I., & Bertevello P.L. Preliminary analysis of hybrid laparoscopic procedure for resection of gastric submucosal tumors. Rev Col Bras Cir. 2016; 43(2), 129–135.[PubMed]
[Free
Full Text]

