Case Report

A Case of Pulmonary Artery Pseudoaneurysm Secondary to Epithelioid Choriocarcinoma
*Hide Wee, *Ali Akbar Fazuludeen, * Keerthi Rajapaksha, * Atasha Asmat, * Dokeu Basheer Aneez Ahmed
- * Department of Thoracic Surgery, Tan Tock Seng Hospital, Singapore
- Submitted: June 28, 2015
- Revised: March 17, 2017
- Accepted: Monday, March 20, 2017
- Published: Friday, March 31, 2017
This is an Open Access article distributed under the terms of
the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
Pulmonary Artery psuedoaneurysms (PAP) can cause significant morbidity and mortality in case of a complication and rupture. PAP caused by the malignant tumours is rare.
Case Presentation
We present a case of 35 year old Chinese women who presented with spontaneous left sided chest pain imaging revealed cavitating lesion in the anterobasal segment of her left lower lobe. She underwent thoracotomy and lobectomy. Histology revealed it to be metastatic choriocarcinoma.
Conclusion
This case illustrates that metastatic carcinoma could be a possible etiology for PAP. Proper pre-treatment evaluation of PAP and pulmonary artery aneurysms necessitates surgical biopsy to rule out malignancy.
Keywords
thoracic, pulmonary artery, pseudoaneurysm, choriocarcinoma
Background
Pulmonary artery pseudaneurysms (PAP) are pulmonary artery dilatations not involving all three layers of the vessel wall. They can cause significant morbidity and mortality in the event of rupture. Causes include infection, trauma and malignancy [1]. Metastatic choriocarcinoma as an etiological factor has not been reported. Choriocarcinomas are malignant gestational trophoblastic disease and is more detrimental in the south-east
Asian population. We present a case of primary ovarian epithelioid choriocarcinoma with pulmonary metastasis resulted in a PAP.
Case description
A 35-year old Chinese female presented with one day of pleuritic left sided chest pain. She denied history of trauma or fever. On examination, we found absent breath sounds on her left hemithorax. A moderate left sided effusion was noted on her chest x-ray. She underwent ultrasound-guided aspiration, which revealed markedly bloodstained fluid.
Computerized tomographic angiogram showed a 2.6X2.4 cm size cavitating lesion in the anterobasal segment of her left lower lobe with an adjacent 2.2X2.0 cm early arterial phase homogeneously enhancing lesion. This was supplied by the apical branch of the inferior pulmonary artery and drained to the inferior pulmonary vein (Figure 1).
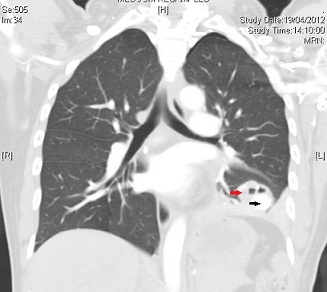
Figure 1: Computerized tomographic angiogram showing the pulmonary artery pseudoaneurysm. supplied by the apical branch of the inferior pulmonary artery and draining into the inferior pulmonary vein. Red arrow indicates tumor, black arrow indicates pseudoaneurysm.s
This is representative of a PAP. The pleural effusion was hyperdense which confirmed its hemorrhagic nature. She was offered the options of interventional embolization versus a thoracotomy and lower lobectomy and opted for the latter. Intraoperatively, we found a 3.0x2x1 cm cystic lesion associated with a 2.2x2.1 cm aneurysm of left lobar pulmonary artery (Figure 2).
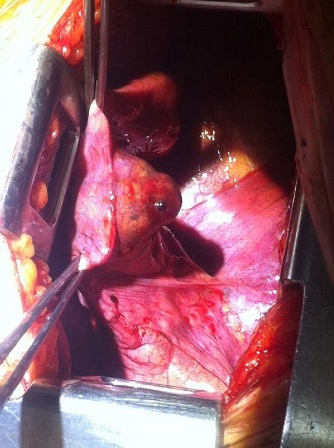
Figure 2: Intraoperative picture of the pulmonary artery pseudoaneurysm
The lesion had central necrosis. Viable tissues consisting of irregular islands of polygonal to spindle cells with enlarged, pleomorphic, hyperchromatic nuclei, prominent nucleoli with dense eosinophilic cytoplasm and intracellular bridges
were present. Keratinization was present and frequent mitotic activity seen. P63 was found to be positive while CK5/6, CD 31, CD34, and TTF-1 were negative. Initial histological diagnosis of a moderately differentiated keratinizing squamous cell carcinoma was made.
Eight months later, she developed a 4 cm erythematous patch on her occiput and underwent excision. Biopsy of this lesion revealed central necrosis similar to the lung lesion. It had a mixture of large cells with vesicular nuclei, distinct nucleoli with fairly well defined cell margins and syncytial type cells, some multinucleated with hyperchromatic nuclei. There was marked nuclear atypia and high mitotic activity. Cells stained positive for beta human chorionic gonadotropin (β HCG), Human placental lactogen (HPL), AE 1/3, CK 7 and EGFR. Focal positivity for placental alkaline phosphatase (PLAP), EMA inhibin and CD 10 was noted.
Following these findings, the lung resection histology was reviewed and its histological features were similar to the occipital lesion, both being immunopositive for β hCG and hPL. As AS 1/3 and CK7 were also positive, this was determined to be a rare variant of metastatic choriocarcinoma with epithelioid features.s
PET CT showed a Flurodeoxyglucose (FDG) avid lesion in her ovary in addition to lung and scalp suggesting that the primary was of ovarian origin. In view of her advanced metastatic disease, she was started on intensive combination chemotherapy.
Discussion
PAPs are a contained rupture of the pulmonary artery. This is in contrast to aneurysms where all layers of the vessel wall are affected. Etiological factors identified include trauma, malignancy, infection and iatrogenic intervention [1- 3]. Malignant causes include both primary lung cancers and metastasis. However metastatic choriocarcinoma has not been previously documented as an etiological factor for PAP. Various pulmonary involvement of choriocarcinoma are described in literature [4-7]. Due to the rarity of the disease and variable presentation, diagnosis is difficult and retrospective diagnosis of the primary malignancy after detection of pulmonary lesion is also frequently documented
[6].
Majority of pulmonary artery aneurysms are treated by watchful waiting, embolization, endovascular stent graft or surgical excision in a form of wedge or lobectomy or surgical vessel ligation. However none of the non-surgical methods provide a histological specimen. As carcinoma is a well-known cause of pulmonary artery aneurysm, evaluation of PAPs for malignancy is important prior to offering catheter-based interventions. At minimum, a PET-CT is necessary to delineate the possible primary sites and other metastatic sites.
Conclusions
This case illustrates that metastatic choriocarcinoma is a possible etiology for PAP. Proper pre-treatment evaluation of PAP and pulmonary artery aneurysms necessitates surgical biopsy or PET-CT to rule out malignancy.
Authors Contributions
HW: Prepared the draft manuscript, literature search.
AAF: preparation of manuscript.
KR: Preparation and editing of manuscript.
AA: Preparation of manuscript.
DBAA: Concept design and editing of the final manuscript for publication.
Ethical Consideration
The written informed consent was taken from the patient for publication of this case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there are no conflicts of interests. This case was presented at ASCTVS 2014 annual conference.
References
[1]. Restrepo CS, Carswell AP, editors. Aneurysms and pseudoaneurysms of the pulmonary vasculature. Semin Ultrasound CT MR. 2012 Dec;33(6):552-66. [PubMed]
[Full text]
[2] Balagopal P, Pandey M, Chandramohan K, Somanathan T, Kumar A. Unusual presentation of choriocarcinoma. World J Surg Oncol. 2003;1(4).[PubMed]
[PMC]
[3]. Lafita V, Borge MA, Demos TC, editors. Pulmonary artery pseudoaneurysm: etiology, presentation, diagnosis, and treatment.
Semin Intervent Radiol. 2007 Mar;24(1):119-23. [Pubmed]
[PMC Full text]
[4] Fatnassi R, Slimene F, Dhouibi S, Karray T, Negra R. [Uterin choriocarcinoma revealed by pulmonary metastasis. A case report]. La Tunisie medicale. 2005;83(10):645-7.[PubMed]
[5]. Parks DG. Maternal and neonatal death from advanced choriocarcinoma due to a delay in diagnosis: a case report. J
Reprod Med. 2007;52(3):228-30 [PubMed]
[6]. Sierra-Bergua B, Sánchez-Marteles M, Cabrerizo-García J, Sanjoaquin-Conde I. Choriocarcinoma with pulmonary and cerebral metastases. Singapore
Med J. 2008;49(10):e286-8 [PubMed]
[7] Zaheer S, Osmany S, Lai HK, Eng DNC. Usefulness of F-18 fluorodeoxyglucose positron emission tomography/computed tomography in a case of choriocarcinoma presenting as pulmonary embolism. Clin
Nucl Med. 2009;34(6):343-5 [PubMed]

