Case Report

A Case of Ectopic Lingual Thyroid: The Importance of Preoperative Vascular Evaluation
1 Nicolas Sigaux, 2Pierre Philouze, 2Alexis Ambrun, 3Frédérique Le Breton, 4Françoise Borson-Chazot, 5Jean-Christian Pignat
- 1Maxillofacial Surgery, Hospices Civils de Lyon, Université Claude Bernard Lyon I
- 2Otorhinolaryngology – Head and Neck Surgery, Hospices Civils de Lyon, Université Claude Bernard Lyon I
- 3Anatomical Pathology, MD, Croix-Rousse Hospital, Hospices Civils de Lyon
- 4Endocrinology, MD PhD, East Hospital,Hospices Civils de Lyon, Université Claude Bernard Lyon I
- 5Otorhinolaryngology – Head and Neck Surgery, MD PhD, Croix-Rousse Hospital, Hospices Civils de Lyon, Université Claude Bernard Lyon I
- Submitted: Tuesday, August 26, 2014
- Accepted: Sunday, October 05, 2014
- Published: Wednesday, October 22, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Symptomatic ectopic lingual thyroid is a rare condition. The purpose of our work is to demonstrate the importance of an accurate clinical, biological and radiological evaluation, in order to decide when and how to treat.
Case presentation
A 55 year old male patient with no history of dysthyroidism presented in outpatient clinic for the management of intermittent episodes of mouth bleeding complicated with anemia. The nasopharyngoscopy revealed a thyroid-looking lump at the base of the tongue, pushing down the epiglottis. Thyroid stimulating hormone was slightly elevated. Technetium-99m scintigraphy and ultrasonography confirmed the absence of thyroid tissue in normal position. CT scan showed a 38x32x16 mm mass, vascularized by a single ectopic artery coming from the right external carotid artery. After 4 years of suppressive medical therapy, a surgical excision was realized with a cervical approach. Safe vascular control of the ectopic gland was guaranteed by CT angiography.
Conclusion
Surgical management of ectopic lingual thyroid is often decided after medical treatment's failure. It requires a precise radiological evaluation, including a CT angiography, looking for an ectopic vascularization and helping to choose the safest surgical approach.
Key words
ectopic thyroid; lingual thyroid; CT angiography
Introduction
Ectopic thyroid is the consequence of failure of the gland to migrate from the foramen caecum to its pre-laryngeal position, occurring between the 3rd and the 7th week of embryological development. Lingual position was first described in 1869 by Hickmann [1], and represents 90% of the cases [2]. Its prevalence is 1 in 100,000 but is probably underestimated, according to post mortem studies finding lingual thyroid tissue in 10% of subjects [3]. It is four times more common in females than in males, and mean age of clinical manifestations is 40 years[4].
The purpose of our work is to demonstrate the importance of an accurate clinical, biological and radiological evaluation, in order to decide when and how to treat.
Case presentation
A 55-year-old male patient with no history of dysthyroidism presented with recurrent mouth bleeding, complicated with anemia and recent darkening of the stools. Further questioning revealed a covered voice, and a long-term history of night obstructive symptoms.
The nasopharyngoscopy revealed a pink lump with blood vessels on its surface, pushing down the epiglottis and occupying most of oropharyngeal space (Figure 1). Cervical palpation could not find any thyroid tissue in physiological position. The initial evaluation included: thyroid function tests, ultrasonography, scintigraphy, computed tomography (CT) scan and CT angiography.

Figure 1 – Endoscopic aspect of the gland, obstructing widely the oropharyngeal space
Thyroid stimulating hormone (TSH) was slightly elevated (7 mU/L, N=0.4-4.4 mU/L), triiodothyronin (T3) and thyroxine (T4) were within normal range. Technetium-99m (Tc99m) scintigraphy showed an intense fixation at the base of the tongue, and none in prelaryngeal position (Figure 2) Cervical ultrasonography confirmed the absence of thyroid in prelaryngeal region. CT scan revealed an exophyticmedial mass in the lower part of the base of the tongue, measuring 38x32x16 mm, containing an area of calcification. After the administration of contrast, the lesion was intensely enhanced (Figure 3). CT angiography identified a single ectopic thyroid artery in a very high position, coming from the right external carotid artery, before the origin of right maxillary artery (Figure 4).

Figure 2 – Tc 99m scintigraphy showing a single zone of intense fixation corresponding to the base of the tongue and the absence of fixation in the prelaryngeal area.
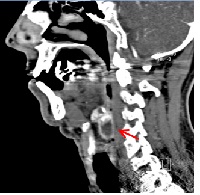
Figure 3 – Contrast-enhanced CT scan, sagittal view The red arrow is pointing to the gland, situated behind hyoid bone.

Figure 4 – CT angiography: right lateral view
1. Ectopic thyroid; 2. Hyoid bone; 3. External carotid artery; 4. Ectopic thyroid artery; 5. Maxillary artery; 6. Superficial temporal artery
A suppressive medical therapy by Levothyroxin was initiated, with a progressively increasing dose. No new episode of bleeding was noticed, and the volume of the mass slightly decreased, once the dose of 125 micrograms was reached. Mean range of TSH was approximately 2.60 mU/L (N= 0.4-4.4 mU/L). After 4 years of treatment and follow-up, due to intensifying obstructive symptoms, a surgical excision was performed. A right cervical transhyoid approach was used, following the path of the right carotid artery, allowing a safe vascular control of the gland. Four lesions were excised; pathological examination reported four individual localization of encapsulated thyroid tissue, measuring from 0.5 to 3 cm. One of them contained areas of calcification; there were no sign of degeneration (Figure 5). No post-operative complication was noticed. Long-term thyroid hormone replacement was needed.
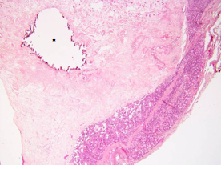
Figure 5 – Microscopic examination of the border of the gland; a dystrophic calcificationis marked with * (magnification x2.5, HES enhancement)
Discussion
Presentation
The most usual symptoms of ectopic lingual thyroid are signs of oropharyngeal obstruction: foreign body sensation in the throat, dysphagia, dysphonia and dyspnea.Ectopic lingual thyroids revealed by episodes of bleeding are very unusual according to our review of the literature. A case of massive bleeding was reported in a pregnant woman, related to a lingual thyroid complicated with adenoma [5].
TSH elevation is frequent in symptomatic lingual thyroid, sometimes accompanied with signs of hypothyroidism[6]. It might be explained by the fact that the beginning of the symptoms is related to a mild hyperplasia.
Ultrasonography, as the most accessible exam, is a useful way to confirm the absence of thyroid tissue in prelaryngeal position, which is observed in 70% of the cases [7 8].Thyroid scintigraphy, using Technetium-99m or Iodine-123, gives further argument for the diagnosis, showing an ectopic uptake corresponding to functioning thyroid tissue.
The aspect of the gland on CT scan is a hyperdense tissue, highly enhanced after contrast injection. It may be combined with nuclear magnetic resonance (NMR), which doesn’t lead to radiation exposure and gives the most precise morphological study of the tongue, though it is more expensive [9]. Needle puncture might be useful for pathological diagnosis. It must be performed under imaging control, given the risk of massive hemorrhage.
Vascularization
Vascular variations concerning ectopic thyroid are rarely described in the literature. Most of the cases reported a vascularization from lateral branches of lingual artery or facial artery[10 11]. Anatomical studies on cadavers found in one subject an ectopic thyroid with a normal bilateral superior thyroid artery but no inferior thyroid artery [12]. Our case reports another type of vascularization, relying on a single ectopic thyroid artery coming from the right external carotid artery.This justifies a precise vascular evaluation by intra-arterial angiography or 3DreformationCT angiography, especially if surgery is needed.
Management
The aim of the management is to reduce obstructive symptoms without leading to acute complications such as massive bleeding and thyrotoxicosis. The different options of treatment may be combined; their indication depends on clinical, biological and radiological results. Multidisciplinary medical and surgical follow-up is necessary.
Medical therapy with low dose of exogenous thyroid hormone is the first treatment to initiate, in case of mild obstructive symptoms, and it can be progressively increased. It has two objectives: reducing the size of the gland and normalizing thyroid function. The effect of suppressive therapy on glandular hypertrophy is very slow and not always significant. Levothyroxine is necessary to reach clinical and biological euthyroid state, as TSH level is often elevated in ectopic thyroid. This is particularly important in children and women of childbearing age, where long term hypothyroidism has dramatic developmental consequences [8]. Surgical excision must be performed when symptoms worsen despite the medical treatment. Euthyroidism is necessary to prevent thyrotoxicosis. The choice between transoral approach, lateral pharyngotomy approach and transhyoid approach is made according to preoperative evaluation results. CT angiography is a precious element at the time of planning the surgical management of lingual thyroid. As vascularization of ectopic gland is very unpredictable, the operator needs an accurate evaluation of the ectopic thyroid vessels in order to prevent hemorrhage.
Embolization of thyroid ectopic vessels might be used. A case of massive bleeding has been reported, requiring an emergent embolization, before planning surgical excision [5]. Radioactive iodine has been described, and can be helpful in case of contraindication to surgical management[13 14].
Conclusion
Lingual thyroid may be revealed by oropharyngeal bleeding. Surgical management is often decided after failure of medical treatment. It requires a precise radiological evaluation, including a CT angiography, looking for an ectopic vascularization and helping to choose the safest surgical approach.
Learning points
-
Mouth bleeding can reveal lingual thyroid.
-
First step of management relies on suppressive hormonal therapy.
-
Surgical excision is needed in case of
failure of medical treatment.
-
Vascular anatomy of ectopic thyroid is
unpredictable.
-
Preoperative vascular imaging (3D
reformation CT angiography) is useful to
prevent hemorrhagic complications.
Acknowledgement
We thank warmly Dr MC Baqué-Juston (Nice University Hospital) for her helpful participation.
Authors’ Contributions
NS: carried out the literature search and prepared the draft manuscript.
PP: carried out the literature search and prepared the draft manuscript.
AA: designed the study and participated in the manuscript preparation.
FLB: participated in illustration.
FBC: participated in reviewing the manuscript.
JCP: conceived the study and edited the final manuscript.
Ethical Consideration
Written informed consent was obtained from the patient for publication of this case report.
Conflict of Interests
The authors declare that there are no conflicts of interests
Funding
None Declared
References
[1].Hickman W. Congenital tumor of the base of the tongue, pressing down the epiglottis on the larynx and causing the death by suffocation sixteen hours after birth. Trans Pathology Soc. London 1869; 20; 160-163
[2].Batsakis J G, El-Naggar AK, Luna MA. Thyroid gland ectopias. Ann OtolRhinolLaryngol. 1996; 105:996-1000.
[3].Sauk JJ Jr. Ectopic lingual thyroid. J
Pathol. 1970; 102:239-43.
[Pubmed]
[4].Kamat MR, Kulkarni JN, Desai PB, Jussawalla DJ. Lingual thyroid: a review of 12 cases. Br J Surg. 1979 Aug; 66(8):537–539
[Pubmed]
[5].Chiu TT, Su CY, Hwang CF, Chien CY, Eng HL. Massive bleeding from an ectopic lingual thyroid follicular adenoma during pregnancy.Am J Otolaryngol. 2002 May-Jun;23(3):185-8.
[Pubmed]
[6].Neinas FW, Gorman CA, Devine KD, Woolner LB. Lingual thyroid: clinical characteristics of 15 cases. Ann Intern Med. 1973; 79(2):205-210.
[Pubmed]
[7].Fish J, Moore RM. Ectopic thyroid tissue and ectopic thyroid carcinoma: a review of the literature and report of a case. Ann Surg. 1963; 157:212- 218
[Pubmed]
[8].Rahbar R, Yoon MJ, Connolly LP, Robson CD, Vargas SO, McGill TJ, Healy GB.Lingual thyroid in children: a rare clinical entity. Laryngoscope. 2008 Jul; 118(7):1174-9.
[Pubmed]
[9].Oueslati S, Douira W, Charada L, Saïd W, Milka N, Rezgui L, Mnif N, Chaabene M. Thyroïdeectopique. Ann OtolaryngolChirCervicofac , 2006 ; 123, 4: 195-198.
[Pubmed]
[10].Bianco MR, La Boria A, Franco T, Ferrise P, Allegra E. Ectopic lingual thyroid with vascular anomalies. Int Med Case Rep J. 2013; 6: 55–58.
[Pubmed]
[11].Banna M, Lasjaunias P. The arteries of the lingual thyroid: angiographic findings and anatomic variations. Am J Neuroradiol. 1990;11(4): 730–732.
[Pubmed]
[12].Ramesh RT, Balakrishnan R, Prakashchandra S, Suresh R. Ectopic thyroid tissue with a rare vascular anomaly. Int J Morphol, 2007, 25(1):121-124.
[13].Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011 ;165 : 375–382.
[Pubmed]
[14].Thomas G, Hoilat R, Daniels JS, Kalagie W. Ectopic lingual thyroid: A case report.Int J Oral Maxillofac Surg. 2003; 32: 219–221[Pubmed]

