Case Report

A Rare Cause of Intestinal Obstruction
*Dr Satendra Kumar,*Dr Seema Khanna *Dr Sanjeev K Gupta
- *Department of general surgery Banaras Hindu University Varanasi
- Submitted: Sunday, 19 February, 2020
- Accepted: Monday, June 1, 2020
- Published:Wednesday, June 10, 2020
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Intestinal obstruction occurring in a Spigelian hernia is an uncommon event in a rare entity. A high index of clinical suspicion is needed to clinch the diagnosis.
Case Report
We report a case of obstructed Spigelian hernia in a 47 year old lady presenting in emergency with a history of swelling in right lower abdomen for four months and non passage of flatus and stool for three days. Contrast-enhanced computed tomography (CECT) of the abdomen was the most accurate radiological investigation. Emergency laparotomy and a tension free mesh hernia repair were done. Post operative course was uneventful.
Conclusions
Spigelian hernia is a rare ventral hernia. The symptomatology is vague but any complication like incarceration or obstruction warrants an emergency exploration. Open or laparoscopic mesh hernioplasty is the treatment of choice.
Keywords:
Spigelian hernia, CECT, Mesh, Hernioplasty
Introduction
Spigelian hernia is an uncommon variety of ventral hernia presenting with vague symptomatology. This usually lies beneath the aponeurosis of the external oblique muscle, which is a relatively tough structure, making the clinical detection difficult. The usual site is the terminal ileum, but it can occur anywhere in the gastrointestinal tract. This type of hernia is more prone to complications and can mimic acute abdominal conditions such as appendicitis, diverticulitis and tubo-ovarian pathology [1]. It may be a cause of ill defined pain in lower abdomen but rarely the patient may present in emergency with intestinal obstruction. We report a case of obstructed Spigelian hernia with ileocaecal region as the content of the hernia sac.
Case Report
A 47 year old lady presented in surgery outpatient department with a history of swelling on right side of abdomen for four months. The swelling was insidious in onset, asymptomatic initially. It gradually progressed over time and attained the present size. It increased on straining and walking and spontaneously reduced in size on lying down. For the last seven days, she developed pain in abdomen, followed by non-passage of flatus and stool for three days and vomiting for one day. Pain was intermittent, mild to moderate in intensity, none radiating. Vomiting was 2-3 episodes in one day, non-projectile, non-bilious, small in amount and contained food particles. There was no history of dyspepsia, altered bowel habits, constipation, malena. There was no history of cough, or hematemesis in the past. The patient had significant post-operative history. She underwent Lower segment caesarian section 25 years back, appendicectomy 6 years back and laparoscopic cholecystectomy 4 years back.
At the time of presentation, her pulse was 106/min, blood pressure of 164/82 mmHg and a respiratory rate of 16/min. She was anaemic, but hydration was adequate. On inspection, abdomen was bulky and flabby, previous surgery scar marks were present, all healed by primary intention. The right iliac fossa appeared to be full, all hernial orifices were intact and there was no visible peristalsis or pulsation. On palpation, diffuse guarding and tenderness was present and a 6x4 cm size lump was palpable in the right iliac fossa. It was tender, firm in consistency, non-reducible, non-compressible and no cough impulse was present. There was no free fluid in the abdomen. Bowel sounds were hyperactive and digital rectal examination revealed an empty rectum. A clinical diagnosis of post appendicectomy obstructed incisional hernia was made. Plain X-ray abdomen showed multiple air-fluid levels consistent with intestinal obstruction. The ultrasound report gave a new dimension to diagnosis. It was reported as textiloma or gossypiboma (Fig 1). The patient had undergone a CECT abdomen which was handed to us later by attendants which showed a large defect in right transverse abdominis aponeurosis just lateral to right rectus abdominis with herniation of caecum and ileocaecal junction along with their mesentry. Proximal small bowels loops were dilated and large bowel was collapsed (Fig2).
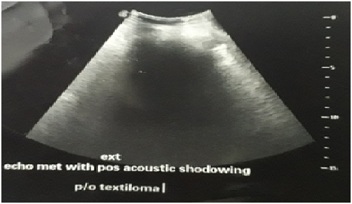

Fig- 1: Ultrasound Image showing an echogenic substance with extensive posterior acoustic shadowing with surrounding mild collection noted in right iliac fossa suggestive of Textiloma

Fig-2 : Large defect in right transverse abdominis aponeurosis with herniation of caecum and ileocaecal junction with dilatation of proximal small bowel loops showing multiple air fluid levels suggestive of Obstructed Spigelian Hernia.
Hence a final diagnosis of obstructed Spigelian hernia was made and patient was taken for emergency laparotomy after optimization for anesthesia. Under general anesthesia an incision was made directly over the bulge in right iliac fossa. Stretched External oblique aponeurosis was visualized with underlying bulge. The aponeurosis was divided. Internal oblique muscle was found to be stretched and a 3 x 3 cm defect was found in transversus abdominis aponeurosis just lateral to rectus sheath infra-umbilically. Hernial sac was delineated and opened at the neck of the sac (Fig 3). The contents were caecum, ileaocaecal junction and omentum (Fig 4). Bowel was healthy. Contents were reduced, sac was excised and muscles sutured in 2 layers. A 15 x 15 cm polypropylene mesh was placed below external oblique aponeurosis. Incision was closed with subcutaneous drain placement. The postoperative course was uneventful. Drain was removed on post operative day 2 and patient was discharged on post operative day 5. Patient was asked to avoid straining and lifting heavy weight and to use abdominal binder for three months. She was referred to cardiology for further management of hypertension. During follow-up of 1month and 6 month she did well and no evidence any complication including recurrence noted.
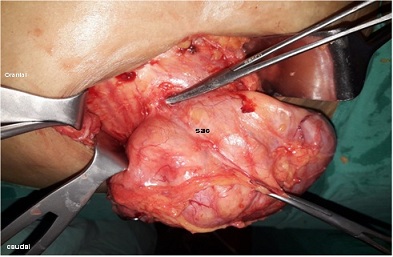

Fig-3: Operative photograph showing hernial sac

Fig-4: Operative Photograph showing Caecum and omentum as content
Discussion:
Spigelian hernia is a rare ventral hernia, the incidence being 0.12% to 2% of all abdominal wall hernias [2]. Adriaen Van den Spieghel, a Belgian anatomist was the first to describe the semilunar line (linea spigele) in 1645. Spigelian hernias occur through a defect in the spigelian aponeurosis, which is the aponeurosis of the transverse abdomines muscle limited by linea semilumaris laterally and lateral edge of rectus muscle medially[3,4].Josef Klinkosch (1704) was the first to describe the spigelian hernia as a defect in the semilunar line [2]. Mostly, they occur in the spigelian hernia belt, a transverse 6 cm wide zone above the line joining the two anterior superior iliac spines. Majority occur at the level of semiarcuate line or the arcuate line of Doughlas [5].
They can occur at any age, but most common in elderly people. They have also been described in infants and may be congenital, reflecting incomplete differentiation of the mesenchymal layers within the abdominal wall. Spigelian hernias are thought to occur at the site of fascial weakness related to perforating vessels [6].The predisposing factors which are found to be associated with spigelian hernias are obesity, previous surgeries, chronic obstructive pulmonary disease and abdominal trauma. Spigelian hernia sac typically transverse the fascia of internal oblique and transversus muscle but rarely penetrate the thick external oblique aponeurosis.The contents of the sac are usually greater omentum, small intestine or sometimes large bowel as in our case. Rarely it may contain acutely inflamed appendix or a Meckle’s diverticulum [6].
The Spigelian hernia is clinically asymptomatic in 90% cases [7]. In majority of the patients, the symptomatology is vague and intermittent. There is a lack of consistent physical signs, hence a high index of clinical suspicion is necessary to arrive at the diagnosis of spigelian hernia [8]. Ultrasonographic examination, being operator dependant, may not be able to give an equivocal diagnosis of spigelian hernia and hence a CT scan is more helpful in arriving at a diagnosis. Moreno-Egea a et al in a series of 28 patients reported a confirmed preoperative diagnosis in only 75% of the cases [9]. In our patient also, the diagnosis was clinched by a CECT only.
The repair of hernia can be accomplished with a transverse incision and a primary repair with a non absorbable suture after reducing the contents of the sac. With the advent of various meshes and minimally invasive techniques, the choice of surgical technique to be employed can be tailored according to the patient profile. David W Larson et al have reported a complication free and recurrence free follow up of 6 years of mesh repair for spigelian hernia[4].
Carter JE in 1992 published the first intraabdominal laparoscopic spigelian hernia repair [7]. But the advocates of open repair were of the opinon that this converts a extraperitoneal surgery to an intraperitoneal one, which has its own complications and side effects. In 1999, A. Moreno-Egea et al published their experience about the totally extraperitoneal laparoscopic approach which avoided the entry into the abdominal cavity [9]. In our opinion, an anterior hernioplasty is a safer option in cases presenting with complications such as obstruction, strangulation or incarceration.When an intraperitoneal sac is present, laparoscopic repair can be performed by intraperitoneal onlay mesh hernioplasty (IPOM) or transabdominal preperitoneal hernioplasty (TAPP) technique.
Conclusion:
Obstructed spigelian hernias are a rare cause of intestinal obstruction. Clinical diagnosis is usually not straight forward and a CT scan is the investigation of choice. Surgery is the modality of treatment. Tension free mesh repair is recommended, either open or laparoscopic.
Learning Points:
1 A history of a reducible swelling in Spigelian belt should raise the suspicion of spigelian hernia.
2 CECT abdomens is the diagnostic modality of choice.
Conflict of Interest
Author declares there is no financial interest or any conflict of interest.
Authors Contribution
Dr S. Kumar: Conducting the literature search and preparation of the manuscript.
Dr S.K. Gupta: Proof reading of the manuscript before submission.
Dr S. Khanna: Finalization of manuscript and also proof reading of the manuscript.
References:
[1].Parambath AN, Hajaji K, Al Hilil SA. Spigelian hernia with Richter-type herniation of the ileum: A rare cause of right iliac fossa pain mimicking acute appendicitis Journal of Emergency Medicine, Trauma and Acute Care. 2012: http://dx.doi.org/10.5339/jemtac.2012.7.
[2].Miller R, Lifschitz O, Mavor E. Incarcerated Spigelian hernia mimicking obstructing colon carcinoma. Hernia. 2008 Feb; 12(1):87-9.[Pubmed]
[3].Spangen L. Spigelian hernia. World J Surg. 1989 Sep-Oct; 13(5):573-80.[PubMed]
[4].Larson DW, Farley DR. Spigelian hernias: repair and outcome for 81 patients. World J Surg. 2002 Oct; 26(10):1277-81.[pubmed]
[5].Artioukh DY, Walker SJ. Spigelian herniae: presentation, diagnosis and treatment. J R Coll Surg Edinb. 1996 Aug; 41(4):241-3.[Pubmed]
[6].Igwe P O, Ibraham N A. Strangulated sliding spigelian hernia: A Case Report. International J of Surgery Case Reports 2018; 53:475-478[pubmed][PMC Full Text]
[7].Lucian W et al. Large Strangulated Spigelian Hernia: Management of an Uncommon Presentation of Abdominal Hernias in Central Uganda. Case Rep Surg. 2019 Oct 13; 2019:8474730. doi: 10.1155/2019/8474730.[Pubmed] [PMC Full Text]
[8].DeMatteo RP, Morris JB, Broderick G. Incidental laparoscopic repair of a spigelian hernia. Surgery. 1994 Apr; 115(4):521-2.[Pubmed]
[9].Moreno-Egea A, Flores B, Girela E, Martín JG, Aguayo JL, Canteras M. Spigelian hernia: bibliographical study and presentation of a series of 28 patients. Hernia. 2002 Dec; 6(4):167-70.[pubmed]
[10].Carter JE, Mizes C. Laparoscopic diagnosis and repair of spigelian hernia:report of a case and technique. Am J Obstet Gynecol. 1992 Jul; 167(1):77-8.[PubMed]

