Case Report

Amyand’s Hernia Presenting as Irreducible Hernia in an Infant
*Ajay Narayan Gangopadhyaya, *Dinesh Gupta,*Shiv Prasad Sharma *Vijayendra Kumar
- *Department of Pediatric SurgeryInstitute of Medical SciencesBanaras Hindu UniversityVaranasi221 005, India
- Submitted: Wednesday, March 19, 2014
- Accepted: Sunday, April 06, 2014
- Published:Saturday, April 19, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License ((http://creativecommons.org/licenses/by/3.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Amyand’s hernia is the presence of a normal or inflamed appendix in an inguinal hernia sac. It is commonly mistaken for an incarcerated or strangulated hernia or torsion of testis. The preoperative diagnosis of this condition is very difficult. Treatment of this condition involves surgical exploration of the involved side with or without appendicectomy. We present a case of a three month old infant presenting with features of irreducible hernia who was found to have inflamed appendix in hernial sac.
Key words
Hernia; appendix; torsion; appendicectomy
Introduction
Amyand’s hernia is the presence of a normal or inflamed vermiform appendix in an inguinal hernia sac. In 1736, Claudius Amyand first described the presence of a perforated appendix in the inguinal hernia of an 11- year-old-boy .[1] It is a relatively rare presentation of appendicitis, with an incidence of less than 1% . [2,4] Appendicitis within an Amyand’s hernia is an even rarer condition, with a published incidence of 0.13% .[5] We report a case of acute appendicitis in hernial sac in a 3 month old infant who presented with features of irreducible hernia.
Case Report
Three month old baby presented with chief complaints of swelling and redness of right inguinoscrotal region for one day. There was no history of fever, vomiting, and abdominal distension, non passage of flatus and stool or trauma. On examination child was lethargic and irritable, with right side inguinoscrotal swelling , which was tender and irreducible. Testis was not separately palpable and cord was thickened. USG inguinoscrotal region showed scrotal oedema with right sided inguinal hernia with normal testis. Haematological investigations showed leucocytosis. Swelling couldn’t be reduced so patient was planned for inguinal exploration. During surgery on opening the hernial sac, an inflamed appendix was found adherent to the sac. [Figure 1,Figure 2,] (Appendicectomy and herniotomy was performed. Postoperative course was uneventful.
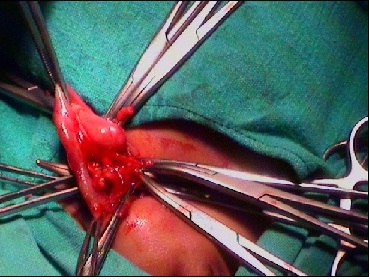
Figure 1
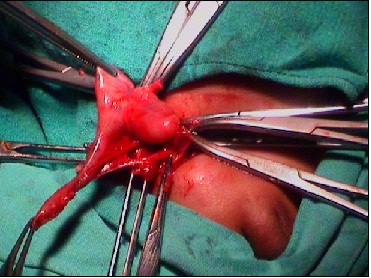
Figure 2
Discussion
Amyand’s hernia is three times more common in children than in adults, probably because of patent processus vaginalis. In infants, acute appendicitis occurs in less than 0.1% of patients. [6] Only less than a quarter of these patients have their appendix incarcerated in a hernial sac. [6] This association may be secondary to the presence of a congenital band that extends from the appendix into the scrotum up to the right testis .[7] Exact pathophysiology of amyand’s hernia is not known. Some authors believe that contraction of abdominal muscles result in entrapment of the appendix leading to compromised blood flow with resultant inflammation and bacterial overgrowth. However, some authors believe that appendicitis is an incidental finding with Amyand’s hernia. [6,8]
Amyand’s hernia is usually confused with an obstructed or strangulated inguinal hernia, torsion of the testis or with epididymo- orchitis. The preoperative diagnosis of this condition is very difficult. Treatment of this condition involves surgical exploration of the involved side with or without appendicectomy. Traditionally, Amyand’s hernia has been treated with open appendectomy and primary hernia repair. However, laparoscopic surgery has also been reported for treatment of this condition. [2]
Conclusion
Amyand’s hernia should be kept in the differential diagnosis of any childpresenting with features of irreducible or strangulated hernia. Prompt treatment can prevent
complications associated with it.
Authors' Contribution
ANG: helped in understanding basic of amyand hernia and
preparation of manuscript.
DG: helped in designing of study
SPC: helped in
data analysis and interpretation
VK: helped in proof reading of study and
approval of final manuscript.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Ethical Considerations
Written informed consent was obtained from next of kin of the patient for publication of this case report.
References
[1].Amyand C . Of an inguinal rupture, with a pin in the appendix caeci encrusted with stone: some observations on wounds in the guts. Phil Trans R Soc Lond. 1736 ;39:329–336
[2].Tycast JF, Kumpf AL, Schwartz TL et al. Amyand’s hernia: a case report describing laparoscopic repair in a pediatric patient. J Pediatr Surg.2008; 43:2112–2114[pubmed]
[3].Ash L, Hatem S, Ramirez GAM et al. Amyand’s hernia: a case report of prospective ct diagnosis in the emergency department. Emerg Radiol.2005; 11: 231–232[pubmed]
[4].Sharma H, Gupta A, Shekhawat NS et al. Amyand’s hernia: a report of 18 consecutive patients over a 15-year period. Hernia. 2007; 11:31–35[pubmed]
[5].Nigri G, Costa G, Valabrega S, Aurello P, D’Angelo F, Bellagamba R, Lauro A, Ramacciato G.A rare presentation of Amyand’s hernia. Case report and review of the literature. Minerva Chir. 2008; 63(2):169–174[pubmed]
[6].Livaditi E, Mavridis G, Christopoulos-Geroulanos G.Amyand’s hernia in premature neonates: report of two cases. Hernia. 2007; 11:547–549[pubmed]
[7].Baldassarre E, Centonze A, Mazzei A et al. Amyand’s hernia in premature twins. Hernia. 2009; 13:229–230[pubmed]
[8].Yazici M, Etensel B, Gu¨rsoy H et al.Infantile Amyand’s hernia. Pediatr Int.2003;45:595–596[pubmed]

