Case Report

.auto-style1 {
list-style-type: square;
}
Clinical Significance of Tortuosity of The Carotid Artery and Higher
Bifurcation: Report of A Case and Review of Literature .
1 Manoj Pandey
- 1Department of Surgical Oncology, Institute of Medical Sciences, Banaras Hindu University, Varanasi 221005, India
- Submitted: December 2, 2016
- Accepted: January 5, 2017
- Published: January 7, 2017
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
An aberrant carotid artery is at risk of injury during routine procedures if the vessel is placed into altered relationship with structures. The incidence of these variations is reported to be between 6-40% in various series.
Case presentation
We present a case of 46 year old male presented with cancer of the buccal mucosa wherein a high bifurcation of carotid artery along with tortuosity of the common carotid and internal carotid artery was found.
Conclusions
the anatomical variations of the carotid vessels can place these vessels at risk of injury at the time of surgery and hence knowledge of these variations is essential.
Key words
carotid artery; external carotid; internal carotid; internal jugular vein; spinal accessory artery; neck dissection.
Introduction
Aberrant course of Internal carotid artery in the temporal bone is often discussed, however, its variations in the neck though not rare are less frequently described [1]. Dr. John Carney of Department of Anatomy, University of Otago, New Zealand in 1924, highlighting this variation and its importance noted that “internal carotid artery may in some cases be tortuous is mentioned in the recent editions of most of our standard textbooks, usually in small type under the heading of peculiarities or of variations” [2]. Quoting Gray (Gray's Anatomy, 22nd edition, p. 625, 1923) he mentioned that, "The course of the artery, instead of being straight, may be very tortuous" and quoting Pierson (Pierson’s Human Anatomy, 7th edition, p. 747, 1919), "In its cervical portion the internal carotid occasionally takes a somewhat sinuous course, and, especially in its upper part, may be thrown into a pronounced horseshoe-shaped curve" [2]. Till 1924 when his paper was published he could identified 12 published reports beside mentions in the textbooks and contributed 36 cases of his own, describing various tortuosities in detail. In an editorial in the same issue [3]. Alejandro Rodriguez Cadarso, and Juan Jose Barcia Guyanese, confirmed the findings of Cairney and added one of their cases. Since, then the various variations of the cervical Internal Carotid artery has been identified and described. We report here one case of aberrant tortuosity of ICA in neck found during neck dissection and discuss its clinical significance.
Case Report
A 46 year old male presented with non healing ulcer on right buccal mucosa. On examination a 4 x 3 cm ulceroproliferative lesion was present in the right buccal mucosa extending from premolar to 3rd molar, both upper and lower gingivobuccal mucosa was free. There were no other abnormalities in the oral cavity. Examination of the neck revealed multiple lymph nodes in level Ia, Ib and II, largest lymph node was 4cm size in level II. Systemic examination was unremarkable. A punch biopsy was taken that showed non keratinizing squamous cell carcinoma. Patient was planned for a surgical excision and hematology and biochemistry was ordered that was found to be normal. A CT scan was performed that showed primary lesion as thickening of the buccal mucosa without any bony involvement and multiple lymph nodes in the right neck.
He underwent wide local excision with right modified radical neck dissection. Intraoperatively the Common carotid artery was found to have tortuous course with curvature to the right coming out underneath the internal juglar vein and then turning left at carotid bulb and bifurcating with external carotid Artery going behind the Internal catotid artery with ansa cervicalis on top of it (Figure 1). Due to presence of this tortuosity of the CCA and high bifurcation with again tortuosity of Internal carotid artery, this came to lie in the plane of dissection, which normally is always lateral to IJV as the arteries are almost always medical to IJV. The patient made fine recovery and was sent home on 5th postoperative day.
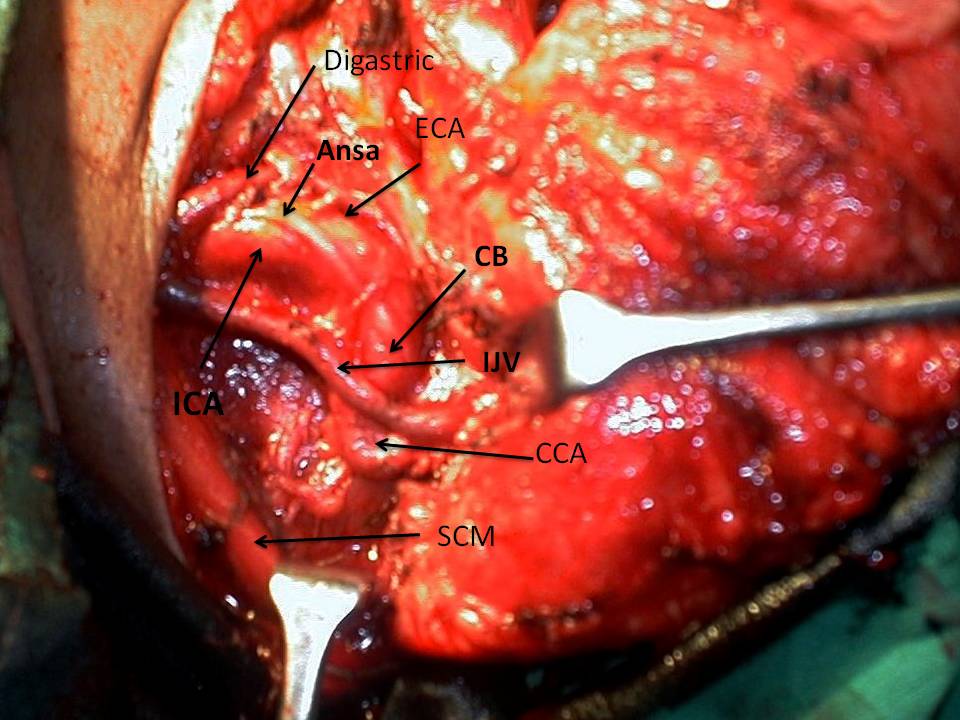
Figure 1: intraoperative photograph showing tortuous common carotid artery, high carotid bifurcation and anomoulous internal carotid artery (ECA-External carotid artery; ICA- Internal carotid artery; CCA- common carotid artery; IJV-Internal jugular vein; SCM- Sternocleidomastoid muscle)
Discussion
Anomalies of the carotid arterial system including the developmental anomalies are not very common and has very high importance for head neck surgeons. According to the classical descriptions the Right CCA arises from the brachicephalic trunk and the carotid bifurcation lies at the level of upper border of thyroid cartilage at C3-C4 vertibral level. The ICA runs straight to skull base, while ECA runs to a point behind mandible giving altogether 8 branches in the neck. However, variations in the anatomy have been reported in 10-40% of the population, most of these variations are minor and does not have much significant clinical relevance [4-10]. On the other hand the variations also present with symptoms and clinical diseases like ischemia and stroke and symptomatic neck masses [11-18]. Pronounced variations may place the vessel in the operating field of the surgeon making it at risk of injury, such can occur during the endoscopic nasal surgery, tonsillar surgery, parapharangeal surgeries and neck dissections for malignancy as in the present case. Anu et al., [18] reported on 95 cadaveric dissections and found higher bifurcation at the level of C2 vertebra in 10% of their cases like the present case. They also reported that in their patients with higher bifurcations some of the arterial supply to the neck like the superior thyroid artery was seen arising from CCA, however in their case the CCA was straight and did not form any loop or show any tortuosity as in the present case [18].
Weibel an Fields in 1965 [19, 20] first introduced a classification system for the variations that is still quite useful. Their work helped to distinguish tortuosity, kinking, and coiling of the carotid arterial system. In 2008, Pfeiffer and Ridder [1] introduced another classification wherein they included the distance from pharangeal wall and the anatomical location as well. This classification is very useful for surgeon while performing parapharangeal surgeries. Out of 265 dissections in the series of Paulsen et al., [5] carotid artery showed no curvature in 191 cases, but in 74 cases it had a medial, lateral or ventrocaudal curve. Desai et al., [21] in a review stated that “The cause of these loops is related to embryological development” they further elaborated that as this arises from 3rd aortic arch its abnormally kinked in the embryo. “Straightening occurs when the fetal heart and large vessels recede in the thoracic cavity. If the embryological state persists, it produces different kinds of undulations, loops, and kinks” [21].
Though described sparingly in the classical literature the interest in the anatomical variations in the carotid arterial system arose after series of injuries during neck, pharangeal, sinus and tonsillar surgeries in 20th centuries and since then almost every variation in the carotid anatomy has been reported, coupled with increasing use of carotid angiography for ischemia and stroke, the incidence of variations are now reported to be as high as 40%. Though over 100 different variations have been described these can still be conveniently into tortuosity, kinks and coils with or without variations of bifurcation. Its importance during the surgery cannot be understated as in the present case a higher bifurcation at the level of C2 vertebra along with the lateral coiling of CCA that brought it lateral to the Internal jugular vein and therefore into the operating field placed it at a risk of injury. This was further compounded by a very laterally placed accessory nerve and posteriomedially curved ECA.
Learning points
-
The anomalies of carotid artery anatomy are present in upto 40% of the patients.
-
These could be in the CCA, ECA or in ICA
-
Bifurcation of the carotid though normally at C3-C4 could be higher at C2 in 10% of the cases
-
The distance from the pharangeal wall also varies to as close as less than 1mm.
-
Its important to know of these variations to prevent injuries during surgery.
Author Contribution
MP: did the literature search and wrote the manuscript.
Conflict of Interest
The authors declare that there are no conflict of interests
Funding
None
References
[1] Pfeiffer J, Ridder GJ. A clinical classification system for aberrant internal carotid arteries. Laryngoscope 2008 November;118(11):1931-6
[Pubmed]
[2] Cairney J. Tortuosity of the Cervical Segment of the Internal Carotid Artery. J Anat 1924 October;59(Pt 1):87-96
[Pubmed]
[3] Cadarso AR. A Rare Case of Tortuosity of the Internal Carotid Artery. J Anat 1925 October;60(Pt 1):119-20
[Pubmed]
[4] Thomson A. Notes on Some Unusual Variations in Human Anatomy. J Anat Physiol 1885 Apr;19 (Pt 3):328 -3219(Pt 3):328-32
[Pubmed]
[5] Paulsen F, Tillmann B, Christofides C, Richter W, Koebke J. Curving and looping of the internal carotid artery in relation to the pharynx: frequency, embryology and clinical implications. J Anat 2000 October;197 Pt 3:373-81.:373-81.[Pubmed]
[6] Ovchinnikov NA, Rao RT, Rao SR. Unilateral congenital elongation of the cervical part of the internal carotid artery with kinking and looping: two case reports and review of the literature. Head Face Med 2007 July 25;3:29.:29.[Pubmed]
[7] Ogretmenoglu O. Asymptomatic looping of the internal carotid artery: a case report. Kulak Burun Bogaz Ihtis Derg 2004;12(5-6):144-6
[Pubmed]
[8] Mumoli N, Cei M. Asymptomatic carotid kinking. Circ J 2008 April;72(4):682-3
[Pubmed]
[9]. Danforth CH. The Heredity of Unilateral Variations in Man. Genetics 1924 May;9(3):199-211.
[Pubmed]
[10] Culligan JA. Buckling and kinking of
the carotid vessels in the neck. Minn Med 1960 October;43:678-83.:678-83
[Pubmed]
[11] Zheng JW, Zhang WL, Fan XD, Zhang ZY. Elongation and tortuosity of the bilateral internal carotid artery presenting as a pulsatile cervical mass: report of a case. J Oral Maxillofac Surg 2007 July;65(7):1370-2
[Pubmed]
[12] Quattlebaum JK, Jr., Upson ET,
Neville RL. Stroke associated with elongation and kinking of the internal carotid artery: report of three cases treated by segmental resection of the carotid artery. Ann Surg 1959 November;150:824-32.:824-32.[Pubmed]
[13] Prokopakis EP, Bourolias CA, Bizaki AJ, Karampekios SK, Velegrakis GA, Bizakis JG. Ectopic internal carotid artery presenting as an oropharyngeal mass. Head Face Med 2008 August 26;4:20.:20[Pubmed]
[14]Munks S, Wallscheid A, Pickuth D. [Variations of the anatomical position of the internal carotid artery as an important differential diagnosis of parapharyngeal tumors]. Laryngorhinootologie 2008 December;87(12):874-7.
[Pubmed]
[15]Milic DJ, Jovanovic MM, Zivic SS, Jankovic RJ. Coiling of the left common carotid artery as a cause of transient ischemic attacks. J Vasc Surg 2007 February;45(2):411-3
[Pubmed]
[16] Freeman TR, Lippitt WH. Carotid artery syndrome due to kinking: surgical treatment in forty-four cases. Am Surg 1962 November;28:745-8.:745-8.
[Pubmed]
[17] Barnes WT, Smedley WP. Carotid
insufficiency, due to elongation and kinking of internal carotid artery. Pa Med
J 1965 September;68:41-3.:41-3.[Pubmed]
[18] Anu VR, Pai MM, Rajalakshmi R, Latha VP, Rajanigandha V, D'Costa S. Clinically-relevant variations of the carotid arterial system. Singapore Med J 2007 June;48(6):566-9.[Pubmed]
[19] Weibel J, Fields WS. Tortuosity,
coiling, and kinking of the internal carotid artery. I. Etiology and
radiographic anatomy. Neurology 1965 January;15:7-18.:7-18 .[Pubmed]
[20]Weibel J, Fields WS. Tortuosity,
coiling, and kinking of the internal carotid artery. II. Relationship of
morphological variation to cerebrovascular insufficiency. Neurology 1965
May;15:462-8.:462-8. [Pubmed].
[21]Desai B, Toole JF. Kinks, coils, and carotids: a review. Stroke 1975 November;6(6):649-53
[Pubmed]


