Case Report

Adrenal metastasis from gallbladder cancer: report of a case and review of literature
* Mridula Shukla,
* Mohan Kumar,
#Manoj Pandey
- Department of *Pathology and #Surgical Oncology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India
- Submitted: Friday, August 5th, 2016
- Accepted:Friday, September 2, 2016
- Published Friday, September 2, 2016
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
Cancer of the gallbladder spreads primarily by local invasion and lymphatic spread, vascular metastasis is rare. Adrenal is a common site of metastasis from cancer of the lung, colon and renal carcinoma, however, metastasis from other cancers is rare.
Case presentation
A 32 year old woman presented with painless progressive jaundice and on imaging was found to have primary carcinoma of the gallbladder with liver invasion, lymphatic metastasis and adrenal mass. Fine needle cytology proved it to be a metastatic lesion from the gallbladder. Patient was treated with palliative chemotherapy.
Conclusions
Adrenal metastasis from cancer of the gallbladder is rare with only two cases being reported in literature previously. Solitary metastasis in resectable tumor should always be surgically removed, however, palliative care is recommended if primary tumor is locally advanced and surgically non resectable.
Key words
Gallbladder; adrenal; metastasis; adenocarcinoma; surgery; adrenalectomy; PET, cytology
Introduction
Cancer of the gallbladder is a common neoplasm of the extrahepatic biliary tract. The tumors often present late when the disease is locally advanced and often cure is not possible [1]. Cancer of the gallbladder spreads primarily by lymphatic invasion, however distant metastasis do occur [2]. When occurs the distant metastasis is often to the liver, lung and peritoneum [3]. The metastasis to other sites is very rare and when occurs it’s often to bone and brain. Though adrenal gland is not an uncommon site of metastasis, the majority of adrenal metastasis arise from primary tumors of the lung [4], however metastasis has been reported from breast [5], colon [6, 7], hepatocellular [8, 9], gastrointestinal stromal tumor (GIST) [10], renal cell [11-14]carcinoma, cervical cancer [15] and lymphoma [16]. The metastasis from gallbladder is very rare; we present here a case of locally advanced unresectable gallbladder cancer with metastasis to right adrenal gland.
Case presentation
A 32 year old female presented to the department of surgical oncology with painless progressive jaundice of one month duration. Examination of the patient revealed pallor and ictrus, there was no cynosis, clubbing or generalized lymphadenopathy. The systemic examination was normal, abdominal examination revealed a hard globular well defined mass in the right hypochondrium, the mass moved with respiration and was continues with liver. There was no organomegaly. Rest of the examination was normal. A clinical diagnosis of carcinoma of the gallbladder was made and patient was investigated. Laboratory examination revealed hemoglobin of 10 g/dl, total bilirubin of 11.5 mg/dl, direct bilirubin of 7.0 mg/dl, AST was 97 IU/L, ALT 69IU/L, and alkaline phosphatase of 239 IU/L. Rest of the hematology and biochemical investigations were normal.
A contrast enhanced computed tomography was carried out that revealed a mass in the gallbladder with infiltration of the liver (Figure 1).
The periportal and pericholedochal nodes were enlarged and portal vein was encased in the tumor (Figure 2), a metastatic lesion was also present in the right adrenal gland (Figure 3).

Figure 1: CT picture showing the primary tumor in the gallbladder with hepatic infiltration

Figure 2: CT showing bulky nodal disease with encasement of the portal vein

Figure 3: CT showing adrenal metastasis
A CT guided biopsy from the gallbladder mass along with FNAC was taken from the adrenal mass. Cytology showed cellular Smear shows cells in monolayered sheets and aggregates. Cells are pleomorphic with moderate cytoplasm and pleomorphic nuclei with prominent nucleoli (Figure 4). A diagnosis of carcinoma of the gallbladder with lymph node and adrenal metastasis was made.
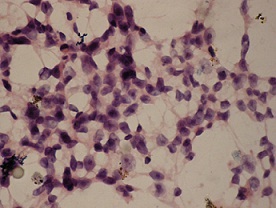
Figure 4: Photomicrograph showing (H &E x400)
As the primary lesion was unresectable, an ERCP was carried out and stenting was tried, however, it failed due to inability to pass the guide wire beyond the obstruction. The patient was started on the chemotherapy using CAPOX protocol with 100mg/m2 oxaliplatin IV on day 1, and capecitabin 1gm/m2 in divided doses for 14 days, with cycle repeated every 3 weeks for 6 cycles. At the end of the chemotherapy, a partial response was noted with tumor regression of 40%. Patient was asked to continue on capecitabine alone. Patient continued on for further three cycles and then was lost to follow-up.
Discussion
The incidence of adrenal metastases from any primary malignancy ranges from 8.6% to 27.0% [17]. The most common primary tumors that metastasize to the adrenal glands is lung, followed by the breast and kidney [4, 18, 19]. Metastasis from gallbladder is very rare with only two previous cases been reported in literature [20, 21]. Both earlier cases have also been reported from India, which has a high incidence of gallbladder cancer. Though rare from gallbladder primary, metastasis to the adrenal are quite common especially from lung cancers, where in it is a routine practice to screen adrenal glands for metastasis along with other abdominal organs. Most of the time the ultrasound is used for screening and has a very high sensitivity for detecting adrenal metastasis, however, the CT scan is being increasingly used.
Recently, 18 fluorodeoxyglucose (FDG) PET/CT is being increasingly used to detect adrenal metastasis. Xu
et al., [22] carried out FDG PET CT for 111 metastatic lesions of the adrenal and reported that a SUV of >2.5 in the adrenal is often suggestive of metastatic tumor. A number of other studies have demonstrated that the detection rate for adrenal glands increases with use of FDG PET [12, 18, 23, 24]. One of the two previously reported case of gallbladder cancer too was diagnosed with FEG PET CT [20]. However, PET CT can not be recommended as evaluation modality in all cancers due to high cost and limited availability specially in third world countries, and hence, ultrasonography and CT scan remains the preferred modality of evaluation.
Mazzaglia et al., [25] reported on the usefulness of biopsy in adrenal masses. Of the total 163 biopsies performed, 88 were for metastatic lesions from various primaries. The rate of malignancy positivity in the biopsy of these 88 metastatic cases was found to be 70%. Highest positivity rate was observed in Lung primaries (90%) followed by renal cell carcinoma (80%), hence they concluded that biopsy should not be performed [25]. However, it is felt that with adrenal incidentloma incidence being high it is important to rule out simultaneous occurrence of a adrenal neoplasm and in such circumstances a core needle biopsy could be of immense value. A number of reports have found cytology to be useful however again the diagnostic yield is higher in metastatic lesion from lung cancer or tumors with characteristic cytological features [26]. Endoscopic ultrasound guided fine needle aspiration and cytology is also being increasingly performed with good diagnostic yield [4, 27].
of metastatic adrenal lesions is controversial. Majority of the literature recommends that if the primary tumor is resectable and adrenal is the only site of metastasis, these should be surgically removed [28]. Surgical resection has been found to increase the survival almost by 3 times compared to patients where no surgical resection is done [29]. In patients where this is not possible or where adrenal is one of the many sites of disseminated metastatic disease, palliative chemotherapy is the treatment of choice. The choice of chemotherapeutic agents is directed by the histological characteristics of the primary tumor. Stereotactic radiation has been successfully used to treat adrenal metastasis from lung cancer [30].
In conclusion, adrenal metastasis from gallbladder cancer is very rare and only 3 cases including the present case have been reported in literature till date. If resectable, surgery is the best modality of treatment, chemotherapy or radiation is reserved for non resectable disease.
Authors' contribution
MS: did the literature search and prepared the draft manuscript.
MK: did the pathology and contributed the pathological part of the manuscript
MP: conceived and designed the study and did the final editing of the manuscript.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Ethical consideration
Written informed consent was obtained from patient for publication of this case report.
Reference
[1].Chao TC, Greager JA: Primary carcinoma of the gallbladder. J Surg Oncol 1991, 46: 215-221 [PubMed]
[2]Dwivedi AN, Pandey M, Shukla RC, Shukla VK, Gaharwar S, Maurya BN: Biological behavior and disease pattern of carcinoma gallbladder shown on 64-slice CT scanner: a hospital-based retrospective observational study and our experience. Indian J Cancer 2012, 49: 303-308 [PubMed]
[3]Pandey M, Aryya NC, Pradhan S, Asthana AK, Gautam A, Shukla VK: Carcinoma of the gallbladder presenting as scalp tumour. Eur J Surg Oncol 1998, 24: 605-607 [PubMed]
[4]Bodtger U, Vilmann P, Clementsen P, Galvis E, Bach K, Skov BG: Clinical impact of endoscopic ultrasound-fine needle aspiration of left adrenal masses in established or suspected lung cancer. J Thorac Oncol 2009, 4: 1485-1489 [PubMed]
[5]. Liu XJ, Shen P, Wang XF, Sun K, Sun FF: Solitary adrenal metastasis from invasive ductal breast cancer: an uncommon finding. World J Surg Oncol 2010, 8:7.: 7.[PubMed]
[6]Capaldi M, Ricci G, Bertolini R, Alessandroni L, Di CA, Saraco E et al.: Colon cancer adrenal metastasis: case report and review of the literature. G Chir 2011, 32: 361-363.[PubMed]
[7]Pascual Piedrola JI, Rincon MA, Tolosa EE, Barba AJ, Romero VL, Rosell CD: [Laparoscopic adrenalectomy for metachronous metastasis. Experience in 12 cases]. Actas Urol Esp 2010, 34: 201-205.
[8]Rubio E, Gonzalez J, Jimenez M, Lucena JL, Gimenez L, Martinez AF et al.: Right adrenal metastases of hepatocarcinoma after liver transplantation: case report and literature review. Transplant Proc 2009, 41: 1067-1069.
[9]. Yamakado K, Anai H, Takaki H, Sakaguchi H, Tanaka T, Kichikawa K et al.: Adrenal metastasis from hepatocellular carcinoma: radiofrequency ablation combined with adrenal arterial chemoembolization in six patients. AJR Am J Roentgenol 2009, 192: W300-W305.[PubMed]
[10]Bashir U, Qureshi A, Khan HA, Uddin N: Gastrointestinal stromal tumor with skeletal muscle, adrenal and cardiac metastases: an unusual occurrence. Indian J Pathol Microbiol 2011, 54: 362-364.[PubMed]
[11]Ishida M, Kojima K, Ohtomo K: Renal cell carcinoma with double synchronous contralateral adrenal metastases. Korean J Urol 2010, 51: 879-881 [PubMed]
[12]. Kumar R, Shamim SA, Shandal V, Sharma P, Gadodia A, Malhotra A: FDG PET/CT in detection of adrenal metastasis in patients with renal cell carcinoma. Clin Nucl Med 2011, 36: 513-517 [PubMed]
[13]McGrogan D, McCavert M, O'Donnell ME, Dolan S: Laparoscopic adrenalectomy for a late solitary renal cell cancer metastasis to the ipsilateral adrenal gland. Ir J Med Sci 2010.[PubMed]
[14]Moslemi MK, Saghafi H, Firoozabadi MH: Renal Cell Carcinoma with Simultaneous Bilateral Adrenal Metastasis: Ipsilateral Radical Nephrectomy with Contralateral Adrenal Preservation. Case Rep Oncol 2010, %19;3: 372-379.
[15]Choi JJ, Buttrick S, Zakashansky K, Nezhat F, Chin EH: Laparoscopic adrenalectomy for isolated adrenal metastasis from cervical squamous cell carcinoma and endometrial adenocarcinoma. Gynecol Oncol 2011, 122: 684-685.[PubMed]
[16]Horiguchi K, Hashimoto K, Hashizume M, Masuo T, Suto M, Okajo J et al.: Primary bilateral adrenal diffuse large B-cell lymphoma demonstrating adrenal failure. Intern Med 2010, 49: 2241-2246.[PubMed]
[17]Villar JM, Moreno P, Ortega J, Bollo E, Ramirez CP, Munoz N et al.: Results of adrenal surgery. Data of a Spanish National Survey. Langenbecks Arch Surg 2010, 395: 837-843 [PubMed]
[18]Lu Y, Xie D, Huang W, Gong H, Yu J: 18F-FDG PET/CT in the evaluation of adrenal masses in lung cancer patients. Neoplasma 2010, 57: 129-134 [PubMed]
[19]Muth A, Persson F, Jansson S, Johanson V, Ahlman H, Wangberg B: Prognostic factors for survival after surgery for adrenal metastasis. Eur J Surg Oncol 2010, 36: 699-704 [PubMed]
[20]Sahoo MK, Sharma P, Suman S, Jain TK, Bal C, Kumar R: Gallbladder carcinoma metastasizing to adrenal gland: a rare site demonstrated with (18)F-FDG PET/CT. Clin Nucl Med 2014, 39: 184-185 [PubMed]
[21]Rawat NS, Negi A, Sangwan S, Sharma U, Thukral BB, Saxena NC: Aggressive adenocarcinoma of gallbladder with distant metastases and venous thrombosis at initial presentation. Indian J Radiol Imaging 2006, 16: 499-501.
[22]. Xu B, Gao J, Cui L, Wang H, Guan Z, Yao S et al.: Characterization of adrenal metastatic cancer using FDG PET/CT. Neoplasma 2012, 59: 92-99.
[23].Basu S, Shet T, Awasare S: Bilateral adrenal metastases and metastatic subcutaneous deposit in the chest wall from osteosarcoma of the mandible: utility of 18F-FDG-PET. Hell J Nucl Med 2009, 12: 51-54.[[PubMed]
[24]Castaldi P, Biondi A, Rausei S, Persiani R, Mirk P, Rufini V: An unusual case of adrenal metastasis from colorectal cancer: computed tomography and fluorine 18-fluoro-deoxy-glucose positron emission tomography-computed tomography features and literature review. Case Rep Oncol 2010, 3: 416-422.
[25]. Mazzaglia PJ, Monchik JM: Limited value of adrenal biopsy in the evaluation of adrenal neoplasm: a decade of experience. Arch Surg 2009, 144: 465-470[PubMed]
[26]Malhotra G, Upadhye TS, Sridhar E, Asopa RV, Garde PS, Gawde S et al.: Unusual case of adrenal and renal metastases from papillary carcinoma of thyroid. Clin Nucl Med 2010, 35: 731-736.[PubMed]
[27]Schuurbiers OC, Tournoy KG, Schoppers HJ, Dijkman BG, Timmers HJ, de Geus-Oei LF et al.: EUS-FNA for the detection of left adrenal metastasis in patients with lung cancer. Lung Cancer 2011, 73: 310-315 [PubMed]
[28]McLean K, Lilienfeld H, Caracciolo JT, Hoffe S, Tourtelot JB, Carter WB: Management of isolated Adrenal Lesions in Cancer Patients. Cancer Control 2011, 18: 113-126 [PubMed]
[29]Iwanami T, Uramoto H, Baba T, Takenaka M, Yokoyama E, Oka S et al.: [Treatment recommendations for adrenal metastasis of non-small cell lung cancer]. Kyobu Geka 2010, 63: 1101-1106 [PubMed]
[30]Holy R, Piroth M, Pinkawa M, Eble MJ: Stereotactic body radiation therapy (SBRT) for treatment of adrenal gland metastases from non-small cell lung cancer. Strahlenther Onkol 2011, 187: 245-251 [PubMed]


