Case Report

Atypical presentation of capillary hemangioma of upper eyelid near the medial canthus: A case report
* Shubhangi Nigwekar,*, Akshay Bhandari,*Pratik Gogri,
- *Department of Ophthalmology, Pravara Institute of Medical Sciences, Loni, Maharashtra, Ahmednagar, India
- Submitted: Thursday, August 14, 2014
- Accepted: Thursday, October 09, 2014
- Published: Wednesday, October 22, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
Capillary hemangioma is a benign vascular tumor composed of proliferating endothelial cells within fibrous tissue. Other names for this tumor include “benign hemangio-endothelioma” and “strawberry nevus.” It is the most common tumor of infancy, occurring in 1 to 2% of infants [1 2] with a female predilection.Capillary hemangioma is a hamartomatous localized proliferation of vascular tissue in a normal location. They manifest by 1-8 months of age. Most hemangiomas regress spontaneously by age of seven years.
Case Presentation
We reported a child of 8 years with gradually increasing mass near medial canthus since 2 months that was found to be capillary haemangioma on histopathological examination.
Conclusion
Steroids, laser and surgical excision are some treatment options. Recurrence after surgical excision can occur in capillary hemangiomas. Atypical late presentation of capillary hemangioma of left upper eyelid is presented in which meticulous surgical excision provided excellent results.
Key words
Capillary hemangioma, Eyelid tumor, hamartomas
Introduction
Capillary hemangioma is one of the most common benign eyelid and orbital tumor in children. It may present as a cutaneous, subcutaneous or deep lesion and usually presents at birth or is evident by 6-8 months of age. The lesion typically manifests within the first few weeks of life, grows rapidly in the first year during the proliferative phase then invariably and slowly regresses over the following 4 to 5 years during the involutionalphase [3-5]. Females are more often affected than males with an approximate ratio of 3 to 1 [4-7]. The tumor can occur on skin, mucous membranes, and in other soft tissues of the body. The most common location in the periocular region is the extraconalsuperonasal quadrant. While capillary hemangioma is usually a clinical diagnosis, orbital ultrasound imaging is especially helpful in subcutaneous and deep lesions to ascertain deeper extension. Most hemangiomas regress spontaneously by age of seven years [1].The choice of treatment depends on lesion location, its size and potential adverse effects of the treatment itself. Steroids, laser and surgical excision are some treatment options.
Case Report
An 8 year old male, presented with painless, progressive mass of right upper eyelid margin near the medial canthus (Figure 1). which was gradually increasing in size since 2 months. Patient was not having any other complaints apart from that. There was no significant medical, surgical, family and birth history. Child was fully immunized as per age.
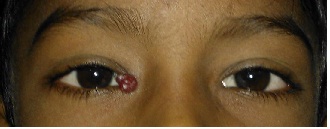
Figure 1:Mass near medial canthus of right eye
General & systemic examination of the patient was normal. Visual acuity of the patient was 6/6 in both eyes. Left eye findings were within normal limits. Local examination of upper eyelid near the medial canthus showed a reddish color lobulated, movable, nontender mass 1 cm in height, width and depth firm in consistency. (Figure 2)There was no crusting, ulceration, bleeding over the mass. Rest of the anterior and posterior segment examination of right eye was normal.

Figure 2:Reddish, lobulated, firm movable mass
A differential diagnosis of pyogenic granuloma or hemangioma was made and total excision biopsy was carried out under general anesthesia and sent for histopathological examination. The skin incision was then sutured with vicryl 6-0, 3 sutures were taken. Histopathological examination of excised lesion shows small to medium sized capillaries and fibrous tissue in the intervening stroma and confirmed diagnosis of capillary hemangioma.(Figure 3)
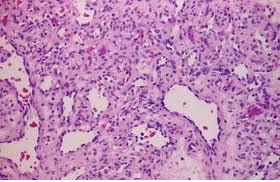
Figure 3: Capillary hemangioma: Histology: varying sizedsmall vascular channels withouttrue encapsulation
Patient was started antibiotic drops and ointment, anti-inflammatory and analgesics drugs post operatively and discharged. Follow up examination after 7 days done. Patient was asymptomatic and there was no lid edema, no discharge.(Figure 4) Sutures were removed on 7th post operative day.

Figure 4: Postoperative view of the patient
Discussion
Capillary hemangioma is a hamartomatous localizedproliferation of vascular tissue in a normal location.Many terms have been used synonymously with “capillary hemangioma”: strawberry hemangioma, strawberry nevus, capillary endothelioma, angioblastichemangioma, hypertrophic hemangioma, and benign hemangio-endothelioma among others. Capillary hemangioma is a tumor of primitive cells with capability to differentiate towards endothelial cells and pericytes. Mast cells are present and play a role in angiogenesis. Microscopic examination of the solid cellular area reveals that the tumor is composed of back-to-back units or groups of cells that consist of endothelial cells and pericytes.One of the most common benign orbitaltumors in children, it affects up to 2 % of all infants,with a female predilection (3:2) [2]. Approximately onethirdof capillary hemangiomas are apparent at birth,while the remaining two-thirds manifest by 6 months ofage.
The history and presentation of a periorbitalcapillary hemangioma is so typical as to be diagnostic.Parents usually describes a growing red or purple spotthat was not present at birth but becomes larger andthicker over the first few months of life. The lesionblanches with pressure, which is helpful indistinguishing it from the non-blanching ‘port-wine’stain of Sturge-Weber syndrome. While mosthemangiomas are not present at birth, more than halfof them will manifest by 1-2 months of age and 90-100% of the lesions will be present by 6-8 months ofage. The peak size of the lesion is reached by 6-12months, at which point the hemangioma, if leftuntreated, will remain stable for some time beforebeginning to involute. In fact, spontaneous involution isthe rule for untreated capillary hemangiomas andprogressive involution continues until 8 years of age.Forty percent of hemangiomas completely regress by4 years of age and 80% completely regress by 8 yearsof age [3].
Hemangiomas often follow the distribution of thefirst and second divisions of the fifth cranial nerve.They are usually unilateral and located on the eyelid orbrow and may result in significant ptosis of an involvedeyelid. Reduced visual acuity may be noted due toptosis or astigmatism. Amblyopia is seen inapproximately 50% of patients with eyelidhemangioma [4]. The lesion may be cutaneous or mayextend to subcutaneous tissue. The subcutaneousportion may extend into the orbit causing painless, nonpulsatingproptosis of the involved eye [5]. The ophthalmologist should be aware that manychildren with periorbital hemangioma may also haveintraorbital extension of the lesion and/or systemicangiogenic lesions (including pulmonary, soft-tissueand/or skin lesions). Orbital imaging with B-scanultrasonography is helpful in determining the posteriorextent of suspicious lesions, while chest or abdominalimaging may uncover other hemangiomas. Somepatients with large visceral capillary hemangiomas maydevelop thrombocytopenia, a condition known asKasabach-Merritt syndrome. Capillary haemangiomawith skin haemorrhages, enchondromata of hands andfeet and bowing of long bones is known as Maffuci’ssyndrome [6].
In most cases, capillary hemangiomas involute spontaneously without intervention and with good resulting cosmesis. On the other hand, visual axis obscuration, strabismus, optic nerve compression and proptosis, which may lead to exposure keratopathy, are all major indications for treatment. Systemic indications include thrombocytopenia and obstruction in oral and nasal passages. Early intervention is beneficial if significant anisometropia develops which may result in non-treatable amblyopia.
1. Use of Corticosteroids:Intralesional, systemic and topical corticosteroidsmay be used as treatment.
2. Surgical excision:Surgery carries the risks associated with generalanesthesia. As the lesion is not encapsulated,surgical excision is often difficult and there is a riskof recurrence
3. Immunomodulator: Vincristine, Cyclophosphamide and Interferon alfa-2a has been used as monotherapy or in combinationwith systemic corticosteroids
[7].
Conclusions
Though capillary hemangioma presents usually at birth and up to 1 year of age, it may present as late as 7 years. Meticulous surgical excision gives good results even in recurrent cases. Eyelid and orbital capillary hemangiomas are treatable vascular lesions. Ophthalmologists should be aware of the ocular complications of this tumor. Early recognition and timely diagnosis and treatment may prevent amblyopia and cosmetic disfigurement.
Authors’ Contribution
AB carried out the literature search and prepared the draft
manuscript, SN and AB carried out the
experiments and interpreted the results, PG designed the study
and performed the analysis, AB and SN
conceived the study, participated in design and edited the final manuscript. All
authors read and approved the final manuscript for submission.
Ethical Consideration
Written consent of the patient was obtained for publication of this study
Conflict of Interests
The authors declare that there are no conflicts of interests
Acknowledgement
None
Funding
None Declared
References
[1].Sihota-Tandon. ‘Parson’s diseases of eye’. 21st edition 2011:456.
[2].Haik BG. Capillary hemangioma. SurvOphthalmol 1994; 38(5):399-426[pubmed]
[3]. Review of Capillary Hemangioma, Peralta RJ, Glavas. New York University and the Manhattan Eye, Ear and Throat Hospital, New York. Eye Net Magazine February 2009.
[4].Basak SK. ‘Essenials of Ophthalmology’, 4th edition 2007: 127.
[5].Capillary Hemangioma right upper eyelid: Case report. JM Graff, Adam Garza, KD Carter, January 31, 2006.
[6].Kanski JJ. ‘Clinical Ophthalmology A Systemic Approach’, 6th edition 2007; 105,189.
[7].Yanoff M. ‘Ophthalmology’ 3rd edition 2009: 1462.
[8].Dermatologic Manifestations of Pyogenic Granuloma (Lobular Capillary Hemangioma) JC Pierson, DM Elston. Medscape 29th April 2010


