Case Report

Multimodal Treatment of Mediastinal Follicular Dendritic Cell Sarcoma: a case report successfully treated
1Stefano Sanna, 1Marco Monteverde, 1Marco Taurchini, 1William Grossi, 2Alessandra Dubini, 1Davide Dell’Amore
- 1Thoracic Department - Thoracic Surgery Unit “G. B. MORGAGNI” Hospital – Forlì – Italy
- 2Department of Pathology “GB MORGAGNI” Hospital – Forlì - Italy
- Submitted: October 26, 2012;
- Accepted: December 17, 2012
- Published: January 16, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Follicular Dendritic Cell Sarcoma (FDCS) is an extremely rare malignant tumour of unknown etiology which, just to its heterogeneity, is not always easily recognized, diagnosed and accurately treated. To date only 49 cases of FDCS are reported in Literature. There could be a difficult differential diagnosis with metastatic carcinoma, ectopic thymoma or primary – metastatic malignant fibrous histiocytoma. Superficial and deep lymph nodes in axilla and more rarely in inguinal sites, are usually involved with aspecific symptoms, very rarely intra-abdominal structures are interested. A mediastinal localization of this tumour is even more rare. An accurate diagnosis is very difficult and is often obtained on surgical specimen and only with immunohistochemical studies. The treatment of first choice for this pathology is surgical excision, whatever is the site of the lesion; radio - chemotherapy could be considered as adiuvant treatment, in case of incomplete excisions, or principal treatment of local recurrences or distant metastases, whose rates vary between 24 and 43% of cases. This combinated therapy seems to be the key of good survival rates. We present a case of a 42 years old young man affected by mediastinal FDCS, successfully treated with surgical complete excision of the mass and radiotherapy.
Keywords
Follicular dendritic cell sarcoma, spindle cell sarcoma, lymph node involvement, mediastinal site, surgical therapy.
Introduction
Follicular Dendritic Cell Sarcoma (FDCS) is an extremely rare malignant neoplasm, originating from follicular dendritic cells, which are non lymphoid, non phagocitic accessory cells of the lymphoid system. [1] Described for the first time in 1986, it occurs almost exclusively in young middle-aged people with a mean age of 43 years [2]. Two-third of the patients presents lymphadenopathies; however, extranodal sites of this pathology are not uncommon [2]. Complete surgical resection is considered the treatment of choice [3,4]. The role of adjuvant therapy is unclear; adjuvant chemotherapy and radiation are indicated, particularly in incomplete excisions or recurrences [3,4]. In this report we present the case of a young man affected by mediastinic FDCS and treated with surgical excision and adjuvant radiotherapy with good result.
Case Report
A 42-years old man presented to the emergency department with complaints of frequent episodes of lipothymia and epileptic strokes. In the anamnesis was present a lichen ruber planus resistant to medical therapy, involving the oral cavity and genitals. A chest radiograph showed large paramediastinic opacity, left-sided, oval-shaped. A thoracic CT scan provided a more accurate image describing a neoformation of 6 cm in diameter contiguous to, but without evidence of epiaortic vessels invasion, with heterogeneous soft-tissue attenuation and multiple calcifications. Important mediastinal lymph adenopathies are concomitant. There was no evidence of lung nodules (Fig.1). A CT-scan-guided percutaneous biopsy was performed confirming the malignancy of the lesion, but not the nature. A brain and abdominal CT and routine blood tests were negative.
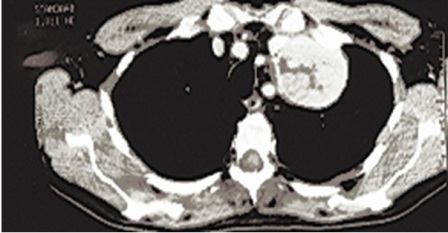
Figure 1: Chest CT scan overview - The Chest Contrast-enhanced CT scan, showed an anterior 6-cm upper left-sided mediastinal neoformation, with regular margins and not homogenous internal pattern, contiguous to the brachiocephalic trunk and the great vessels of the neck.
The patient underwent a left postero-lateral thoracotomy, with identification of an encapsuled 6 cm mass in the upper-anterior mediastinum, extending into the left pleural cavity and up towards the upper thoracic outlet. Preserving accurately the left phrenic nerve, the mass was removed with a systematic lymphadenectomy of 5, 6, 7, and 9 lymph node stations.

Figure 2: Mediastinal follicular dendritic cell sarcoma: hystologic pattern. EE 20x –. Fascicular structures composed by spindle to oval shaped cells proliferation.
Histopatologic assessment of resected specimen showed a partially encapsulated mass, composed by a proliferation of oval to spindled cells forming mainly fascicular structures, few nests and sometimes a storiform pattern. (Fig. 2) The neoplastic cells contained oval nuclei with a bland, vescicular chromatin pattern and inconspicuous nucleoli. The cytoplasm was pale to slightly eosinophilic. The mitotic rate was low. Immunohistochemical staining showed a strongly positivity for vimentine, CD 45RB, CD68 and S-100, only focal and weak positivity for CD35 and CD21 (Fig. 3a-b). These findings were considered diagnostic of Follicular Dendritic Cell Sarcoma.
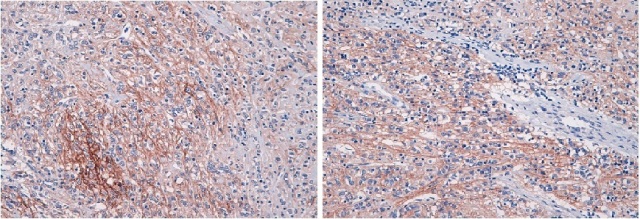
Figure 3: Mediastinal Follicular Dendritic Cell Sarcoma: Immunophenotype 20x: CD21 (a) and CD35 (b) positivity for follicular dendritic markers.
All lymph nodes specimens were negative for neoplastic ìinvolvement.
There were no post-operative complications and the patient was discharged from the hospital in 7th post-operative day. A radiotherapic treatment (25 applications) was decided by oncologists to sterilize the mediastinal field and actually the patient is alive, disease free after a 20-months follow-up.
Discussion
FDCS is an extremely rare neoplasm arising from primary and secondary lymphoid follicles that, owing to its heterogeneity, is not always easily recognized, accurately diagnosed and promptly treated [5]. The first description of dendritic cells was made by Maximow in 1927 [6], who defined the figure of "non-phagocytic embrio-reticular cells" situated within B area of normal lymph nodes. After more than 50 years, Lennert [7] suggested that these cells may constitute the origin of follicular dendritic cell sarcoma. Thus it was only in 1986 that this rare tumour was fully described and characterized by Monda et al., [8], who reported 4 cases involving latero-cervical lymph nodes, underlying that it may be misinterpreted as a form of metastatic carcinoma, ectopic thymoma or primary – metastatic malignant fibrous histiocytoma. This neoplasm generally affects young middle-aged adults [2] without sex predilection, usually presenting as a solitary mass or painless cervical lymphadenopathy in coalescent masses. [8] Superficial and deep lymph nodes are the most frequent sites of follicular cell sarcoma, involving axillar and, more rarely, inguinal lymph nodes, but FDCS have also been known to occur in other locations such tonsils, upper digestive tract, spleen, retroperitoneum and mesenterium [2,4,5].
As concerning the pathology these lesions are variable in size (1-13 cm), usually encapsulated, with three morphologic primary cellular patterns: follicular dendritic cells, reticular-dendritic cells and follicular-reticular dendritic cells. [5] It has been reported some cases of concomitant arise of the tumour with foci of Castleman’s disease and some authors argue that FDCS actually develops from Castleman’s disease as a hyperplasia-dysplasia-neoplasia sequence [9].
To date there have been 49 cases of FDCS reported in Literature, but Perez-Ordonez et al., [2] reported only 3 cases of mediastinal involvement.
From a clinical point of view, some of the cases are asymptomatic as like as our patient the others present problems relating to the compression of the anatomic structures closely to the mass. [4] Sometimes it could be associated with hematologic, neurologic or dermatologic pathologies as multiclonal gammopathy [10] or epilepsy and lichen ruben planus, as in our case, that conduct the patient to the hospital. [4] In most of the cases, as in our observation, the thoracic neoplasm was an occasional radiographic finding. [1,4] Leipsic et al., [4] described the radiologic findings of this neoplasm, showing a large mass on chest radiograph and a large lobulated soft-tissue attenuation mass with foci of course and chunk-like calcification on CT. It’s important to consider intravenous contrast administration to show vascular structures involvement and to assess a correct surgical plan.
As its name implies, FDCS behave like a low-grade sarcoma and a complete surgical resection is considered the treatment of choice. Most of the authors consider safe a radical resection of the tumour with loco-regional lymphadenectomy [1,4,5].
Regarding metastatic disease, FDCS presents an intermediate degree of malignancy, metastasizing in 24 - 43% of cases, mainly to lymph nodes, lungs and liver and bone marrow, occasionally with very long disease-free interval (also 7 years). [5, 11] Lin et al., [12] reviewed 47 reported cases and found that 36% of them developed local recurrence and 27% distal metastases. The prognosis of FDCS is very variable. There were identified some poor prognostic factors as intra-abdominal localization of disease, extensive coagulative necrosis, high proliferation index and presence of significant cell atypia [4,5,9].
The role of adjuvant therapy (chemotherapy and radiation) is still unclear due to the rarity of the tumour. There is common agreement to propose radio and chemotherapy as adjuvant treatment, particularly for patients with post-operative residual disease or metastases [1,4,5].
Conclusion
In conclusion the Follicular Dendritic Cells Sarcoma is a rare neoplasm, with difficult differential diagnosis in which a complete surgical resection is safe and useful. Adjuvant therapy could complete the resection, avoiding local recurrence and metastases. We believe that a major number of cases, a prompt diagnosis and a longer follow-up of treated patients will result in more effective management of this disease.
Authors' Contribution
SS: Wrote the paper and he’s corresponding author.
MM: Collected the case with exams and wrote the case description.
MT: Collected the radiological and operative images.
AD: Reviewed the pathological specimens and wrote the pathological description.
WG: Collected the references in the literature and reviewed it with the corresponding author.
DD: Chief of Thoracic Surgery Unit, read, corrected and approved the manuscript.
All the Authors read, corrected and approved the paper.
Conflict of Interests
None declared
Ethical Considerations
As ethical consideration we didn’t use any experimental drug or technique and, at intervention time, received the complete consensus of the patient about the use of his data and all material about his pathology (images, histologic specimens, etc).
Funding
We have no financial interest in the products presented in this work or any funding to promote and realize the paper.
Acknowledgement
None
References
[1]. Pileri SA, Grogan TM, Harris NL et al. Tumors of the histiocytes and accessory dendritic cells: an immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology 2002; 41: 1-29. [Pubmed].
[2]. Perez-Ordonez B, Erlandson RA, Rosai J. Follicular dendritic cell tumor: report of 13 additional cases of a distinctive entity. Am. J. Surg. Pathol. 1996; 20: 944-55. [Pubmed].
[3]. Cano JR, Cerezo F, Gonzàlez A, Marchal T, Salvatierra A. Follicular dendritic cell tumour of the anterior mediastinum. Cir Esp 2009; 85: 254-6. [Pubmed].
[4]. Leipsic JA, McAdams HP, Sporn TA. Follicular Dendritic Cell Sarcoma of the Mediastinum. AJR 2007; 188: w554-6. [Pubmed].
[5]. Chan JKC Proliferative lesions of follicular dendritic cells: an overview, including a detailed account of follicular dendritic cell sarcoma, a neoplasm with many faces and uncommon etiologic associations. Adv Anat Pathol 1997; 4(6): 387-411.
[6]. Maximow A :Bindegewebe und blutbildende Gewebe, Handbuch der mikroskopischen Anatomie des Menschen. Vol. II/I Edited by W. Von Mollendorff. Berlin, Springer 1927, pp. 232-583.
[7]. Lennert K Malignant linphomas other than Hodkin's desease Histology, cytology; ultrastructure, Immunology. Berlin, Springer-Verlag. 1978: 59-65.
[8]. Monda L, Warnke R, Rosai J. A primary lymph node malignancy with features suggestive of dendritic reticulum cell differentiation. Am. J. Pathol. 1986; 122: 562-72. [Pubmed].
[9]. Chang JK, Fletcher CD, Nayler SJ, Cooper K Follicular dendritic cell sarcoma: Clinicopathologic Analisis of 17 cases suggesting a malignant potential higher than currently recognized. Cancer 1997; 79: 294-313. [Pubmed].
[10]. Michal M, Koza V, Jindra P: Spindle Cell Tumour of lymphonode of probable reticulum cell origin associated with multiclonal gammopathy. Zentralb Pathol 1994; 140: 165-72. [Pubmed].
[11]. Jiang L, Admirand JH, Moran C, Ford RJ, Bueso-Ramos CE. Mediastinal follicular dendritic cell sarcoma involving bome marrow: a case report and review of the literature. Ann Diagn Pathol 2006; 10:357-62. [Pubmed].
[12]. Lin O, Frizzera G. Angiomyoid and follicular dendritic cell proliferative lesions in Castleman’s disease of hyaline-vascular type: a study of 10 cases. Am J Surg Pathol 1997; 21: 1295-1306. [Pubmed].


