Original Article

Assessment on the Quality Of Life of Breast Cancer Patients Undergoing Radiation Treatment in Ghana
*,Kofi Adesi Kyei, *Siaw Doris Oppong, *Samuel Yaw Opoku, *William K. Antwi Samuel Tagoe
- *Department of Radiography, College of Health Sciences, Greater Accra, Accra, Ghana
- Submitted Wednesday, April 30, 2014
- Accepted:Tuesday, June 10, 2014
- Published Monday, June 16, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Objective
the primary aim of the study was to assess factors that contribute to the quality of life of breast cancer patient undergoing treatment to determine the overall quality of life and to suggest ways and methods to improve the situation.
Method
Ninety breast cancer patients referred to the Oncology Unit were conveniently sampled within a three month period. Quality of life assessment was performed using the Functional Assessment of Cancer Therapy (FACT-B) - Specific Scale for breast cancer version 4. Data was analyzed using Statistical Package for Social Sciences (SPSS) version 16.
Results
The peak incidence age was between (56-65) years, 60% had triple modality treatment; thus had undergone surgery and were on chemotherapy and radiotherapy. Seventeen percent had surgery and were on chemotherapy only, 10% had surgery and were on radiotherapy only, 10% had surgery and only one patient was on chemotherapy and radiotherapy. The scores for the quality of life domains were General Emotional (GE) well-being (18.8±8.4), General Physical (GP) well-being (16.5±6.1), General Social (GS) well-being (14.3±7.0) and General Functional (GF) well-being (10.9±5.7). Seventy percent of the patient had stable quality of life, 10% had poor quality of life and 20% had good quality of life.
Conclusion
Considering the quality of life domains or subscale scores and the overall quality of life scores of the patients, it can be concluded that there is no significant difference (p>0.05) in the quality of life of breast cancer patients who receive treatment at the Unit.
Key words
Treatment modalities, Quality of life Subscale, Functional Assessment of Cancer Therapy.
Introduction
World statistics show that, 1.1 million women are diagnosed annually with breast cancer and 410,000 women die from the disease [1]. In Ghana, breast cancer is the leading malignancy which accounts for 15.4% of all malignancies and appears to be on the increase [2].
Quality of life (QoL), a multidimensional construct and an important concept, has, for many years, proven difficult to define [3].
World Health Organization defines QoL as an individualb�s perceptions of their position in life, in the context of the cultural and value systems in which they live and in relation to their goals, expectations, standards and concerns make up their QoL [4]. Ferell on the other hand sees it as a subjective, multidimensional construct, representing functional status, psychological well-being, health perceptions and disease and treatment related symptoms [5]. Although the definitions of quality of life vary, most would agree that it should include the following areas: physical, social/family, emotional and functioning well-being.
QoL is increasingly used as an outcome measure in oncology research studies [6], appearing in a variety of forms in numerous different publications. QoL measures may provide descriptive information about patients with cancer and allow exploring the relationships between QoL and socio-demographic factors (i.e. sex, age, social situation, and education level). Other investigations focus on differences in QoL between groups of cancer patients classified by various characteristics such as disease stage [7], prognosis [8] and treatment [9].
However, most studies look at the influence of treatment on QoL, either to determine the impact of a particular intervention or to explore which of the several has a better effect. The efficacy of new therapeutic interventions is now evaluated in terms of their impact on both quantity and QoL, with the aim of extending survival and improving quality of life. QoL scores can also be used to predict survival, as the better they are, the longer the patient is likely to live [10]. All such studies to date have been conducted in populations with established cancer diagnoses.
Surgery, radiation therapy and systemic therapy are the standard forms of breast cancer therapy either alone or in combination [11].
Cancer patients enter into therapy with the hope of receiving cure only to realize these treatments are often followed by side effects that have negative impact on their quality of life. These treatments accompanied by side effects together with symptoms of the disease may clinically and psychologically affect the total wellbeing of the patient [12] hence the need to assess quality of life.
Measuring QoL in breast cancer has been the focus of clinical practice and research in recent decades which is important in assessing treatment outcome [13]. This could be due to increasing number of breast cancer patients. Also breast cancer may affects womenb�s identity and it is believed that women play important role in the family thus when a woman develop breast cancer the whole family is affected [14], hence studying quality of life in breast cancer patients is vital.
Objectives
1) Assess factors that contribute to the quality of life of breast cancer patients undergoing treatment
2) To determine the overall quality of life and to
3) Suggest ways and methods to improve the situation
Patients and Methods
A retrospective, cross-sectional descriptive approach was used for the study. Ninety patients were conveniently sampled and study was conducted within a period of 3 months. The Functional Assessment of Cancer Therapy (FACT-B) - Specific Scale for breast cancer was used as the survey instrument [15]. It comprises the functional assessment of cancer therapy (FACT-G)-general scale and an additional questions specific to breast cancer patients. The FACT-G instrument addresses domains applicable to patients living with a wide variety of cancers and other chronic illnesses.
The FACT-B (version 4) is a 37-item self-report instrument subdivided into four primary QoL domains and a disease specific domain [15]: functional, physical, emotional and social/family well-being of 27-items and 10 additional items for breast cancer.
Sample Size Determination
The formulae used for sample size determination was n= [Z2 (p) (1-p)]/ (E)2 Where: n = the minimum sample size,Z = the standard score for confidence level (95%), E = the allowable error of 0.05 and P = the sample proportion, (95/220) = (0.430)n= [0.952x0.430 (1-0.430)]/0.052, n= 88.
On the average, 30-32 new patients undergo radiation treatment monthly at the outpatient radiotherapy department. A total of 95 patients in 3 months were obtained on the average. A sample size of 90 patients was chosen to represent 95.0% of the total number of patients undergoing treatment for the 3-months period. The population of patients for the three month was 220 according to data from the department, some of these patients attend for chemotherapy, brachytherapy and 95 of them were undergoing radiation therapy
Hypothesis Testing
Radiotherapy treatment for breast cancer has its related side effects and its quality of life
A hypothesis that was used was:
Ho - Null hypothesis,
Ho: There is no significant difference between the quality of life of patients undergoing treatment in week two as against week four after start of treatment.
H1 - Alternative hypothesis
H1: There is a significant difference between of the quality of life of patients undergoing treatment as against those who have completed the treatment regime
This could be denoted as:
µo = the mean of the quality of life created by treatment regimes.
µ1= the mean of the quality of life created by post treatment regimes.
Then: Ho: µo =µ1,
H1: µo ≠ µ1
Eligible patients, who had received treatment for two weeks or more as well as those for review after completion of treatment, were administered survey questionnaire to complete after the purpose of the study and the nature of participation explained to them and they had consented to participate. Patients who had difficulty in completing the questionnaire were guided by the researcher to understand the questions before answering.
|
Treatment type
|
Mean quality of life score
|
Standard deviation
|
|
Triple Modality
|
78.9
|
22.9
|
|
Surgery + Chemo.
|
81.4
|
17.8
|
|
Surgery + Radio.
|
87.7
|
14.0
|
|
Chemo + Radio.
|
43
|
0.0
|
|
Surgery Only
|
80.3
|
21.5
|
Approval for the study was obtained from the research ethics committee of a higher education institution. The ethics approval was supported by written permission for the study to be conducted at the study site with the ethical standard of confidentiality being upheld. All study participants gave informed consent prior to the commencement of the study and each data collection activity.
Results
Ninety (90) breast cancer patients receiving treatment were recruited for this study and all 90 completed the questionnaire. 97% (87/90) of the respondents were females 3% (3/90) being males. Forty three percent (39/90) were married, 27% (24/90) were divorced, 17% (15/90) were single and 13 % (12/90) were widowed. In all, 43% (39/90) of the respondents were traders, 20% (18/90) were retired.
|
Code Number
|
Mean
|
Standard Deviation
|
|
GP
|
48.9
|
6.1
|
|
GS
|
42.9
|
7.0
|
|
GE
|
56.4
|
8.4
|
|
GF
|
32.7
|
5.7
|
The age distribution ranged between 26 and 95 years with a mean age (59.3±1.5) of years. Majority 60%(18/30) of the respondents were between the ages of 46-65 whiles 13.3% (4/30) were below 45 with 1.7% (8/30) above 66 years.
Abbreviation
GF7 - I am content with my quality of life right now. QoL- Quality of Life
Table 3: Mean Quality of Life scores among patient under the different treatment
modalities
|
Treatment type
|
Mean quality of life score
|
Standard deviation
|
|
Triple Modality
|
78.9
|
22.9
|
|
Surgery + Chemo.
|
81.4
|
17.8
|
|
Surgery + Radio.
|
87.7
|
14.0
|
|
Chemo + Radio.
|
43
|
0.0
|
|
Surgery Only
|
80.3
|
21.5
|
Majority 70% (63/90) of the respondent have Stable QoL whiles 20% (18/90) and 10% (9/90) have Good QoL and Stable QoL respectively.
Although most of the mean quality of life score is in the stable QoL category (50-99), respondents who have undergone surgery and were receiving radiotherapy recorded the highest (87.7± 14.0). Respondents on chemotherapy and radiotherapy only recorded the least
[43].
Abbreviation
GP - General Physical Well-Being question, GS - General Social/Family Well-Being question, GE- General Emotional Well-Being question, GF- General Functional Well-Being question, From the above table, GE (56.4 + 8.4) has the highest response category whilst GF recorded the least response category (32.7 + 5.7). The average values indicate that there is significant difference in the response categoriesAlthough most of the mean quality of life score is in the stable QoL category (50-99), respondents who have undergone surgery and were receiving radiotherapy recorded the highest (87.7 + 14.0). Respondents on chemotherapy and radiotherapy only recorded the least
[43] (Table 4).
|
Variables
|
Items
|
Number of Respondents (%)
|
|
Treatment Type
|
Triple modality
|
54 (60)
|
|
|
Surgery + Chemo.
|
15 (16.7)
|
|
|
Surgery + Radio.
|
9 (10.0)
|
|
|
Chemo. + Radio.
|
3 (3.3)
|
|
|
Surgery Only
|
9 (10.0)
|
Majority 60% (54/90) of the respondents were on triple treatment modality. Only 10% (3/90) was on chemotherapy and radiotherapy
(Table 5).
|
Categorical
Groupings of QoL
|
Frequency
|
Percentage
|
|
Poor QoL
|
0 - 49
|
9
|
10
|
|
Stable QoL
|
50-99
|
63
|
70
|
|
Good QoL
|
100 - 148
|
18
|
20
|
Abbreviation; QoL- Quality of Life
Majority 70% (21/30) of the respondent have Stable QoL whiles 20% (6/30) and 10% (3/30) have Good QoL and Stable QoL respectively.
Discussion
From the results, it was evident that incidence of breast cancer increases with age and then drops at a peak of (56-65) years [Figure.1] This supports the assertion that the chances of getting breast cancer increases with age especially patients in their middle age and those progressing to their old age [16]. The female to male ratio in this study was 10:1 but according to ACS [17], the incidence is 100:1 indicating that it is on the increase at the study site and probably as result of the time of study when many male patients were seen. One observation made during the study was that a number of males were getting aware of the disease and as a result had increased the rate at which they were diagnosed.

Figure 1: Percentage age distribution of respondents (n=90)
Patients interpreted their feelings of wellbeing using expectations, perception, experience and religious or community beliefs. Each of these may vary and each depends on the patientsb� attitude and the specific therapeutic intervention.
There was high responds for the emotional wellbeing section. During the study it was observed that most of the patient answered this based on their faith and believes. It was not surprising that all the respondents were either Christians or Moslems. As one patient puts it b�God knows why this happened to me, may be he is just testing my faith as it happened to Job in the bible. I believe I am healed just that it has not appeared physically and I therefore do not worry about dyingb�.
There were others that believe the disease is not natural and that it is as a result of some b�supernatural forceb� working against them.
An individualb�s ability to perform normal daily activities (i.e. physical, psychological, social, and spiritual domains of life), to meet basic needs, fulfill usual roles, and maintain health is essential [18] rest on his ability to work and marry. But according results (Table 1), majority of the respondents were not able to work including even working at home. Also they did not enjoy life including the things they usually do for fun. These might be the reasons why the functional well being results were low.
The slightly high score in this section (Table 2)suggest that most of the patients had support from their family and were satisfied with family communication about the illness. This may be as a result of the very nature of the culture of Africans, more specifically Ghanaians in which most extended family members are involved in almost every issue regarding individual members of the family. Thereby encouraging and supporting each other in times of trouble and ill health, hence most patients never lose the fight against the disease [19]
The high score seen at the physical well-being section suggest that most of the patients did not fall ill, were not forced to spend time in bed and did not have nausea. (Table 3)
Overall Quality Of Life
Majority of the patient had stable quality of life (Figure.2). This was as a result of patientsb� overall stable quality of life domains. Different treatment types affect quality of life differently. All the patients had stable quality of life except those receiving concomitant treatment (chemotherapy and radiotherapy) where the results may change as a result of the chemotherapy (Figure.3).
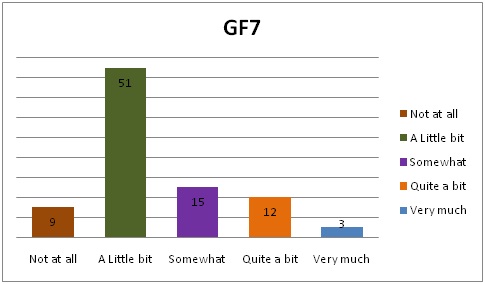
Figure 2: Respondents'� contentment with their QoL

Figure 3: Respondents'� quality of life under the various categories
Patients who had undergone surgery and were receiving radiotherapy had the highest mean quality of life score (87.7) followed by patients who were receiving chemotherapy after surgery (81.4) and finally (80.3) for patients who have had surgery only patient who have had surgery and were currently receiving chemotherapy and radiotherapy had the least quality of life (78.9) (Figure.4).
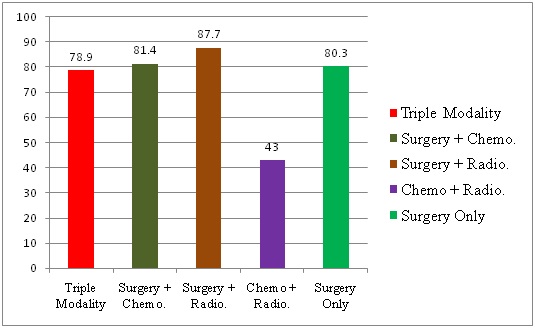
Figure 4: Mean quality of life score for the different treatment modalities
Conclusions
The overall quality of life of the breast cancer patients that presented at the Oncology Unit had very stable QoL. The female to male ratio was 10:1 and the peak incidence age range was between (56-65) years.
Caregivers are entreated to be ready to listen to patientsb� complains and grievances at any point in time during their treatment regime. Also, clinicians and oncologist are entreated to ensure the very best form of treatment is given to breast cancer patients to improve their basic symptoms and the side effects of their treatment in order to enhance their total well-being. Finally, proper education should be given to patients with breast cancer before any form of treatment is given to help increase their quality of life.
Authors' Contributions
DOS and KAK, carried out the literature and prepared the
draft manuscript,
SYO and WKA carried out the experiment and SA interpreted
the results,
KAK and DOS designed the study and performed the analyses
SYO
and SA conceived the study and participated in the study design and
KAK
edited the final manuscript
All authors read the script carefully and
approved the final manuscript for submission
Ethical Considerations
The study was approved by the institute ethics committee.
Conflict of interests
The authors declare that there are no conflicts of interests
Funding
None declared
Acknowledgement
None
References
[1].Stewart BW, Paul, KP. World cancer report Lyon, France, International Agency of Research on Cancer, 2003; 8:100-111.
[2].Badoe EA, Baako. BN. The Breast; Principle and Pathology in the topic Accra. Department of Surgery, Ghana Medical Journal, 2000; 449-477.
[3].3Bottomley A. The Cancer Patient and Quality of Life. European Organization for Research and Treatment of Cancer (EORTC) Data Centre. The Oncologist, 2002; 120-125.[Pubmed]
[4].World Health Organization, 2006. http://www.who.int/whr/2006/en/
[5].Ferrell BR, Dow KH, Grant M. Measurement of the quality of life in cancer survivors. Quality of Life Research, 1996; 4:523-531.[Pubmed]
[6].Giesler RB. Assessing the quality of life in patients with cancer. Current Problem in Cancer, 2000; 24:58-92[Pubmed]
[7].Lakusta CM, Atkinson MJ, Robinson JW, et al. Quality of life in ovarian cancer patients receiving chemotherapy. Gynecological Oncology, 2001; 81:490-495.[Pubmed]
[8].Ringdal GI, Ringdal K. A follow-up study of the quality of life in cancer patients with different prognoses. Quality of Life Research 1998; 9:65-73[Pubmed]
[9].MagnC) N, Marcy PY, Chamorey E, et al. Concomitant twice-a-day radiotherapy and chemotherapy in unresectable head and neck cancer patients: a long-term quality of life analysis. Head Neck, 2001; 23(8): 678-682[Pubmed]
[10].Ganz PA. Quality of life and the patient with cancer. Individual and policy implications Cancer, 2001; 74:1445-1452[Pubmed]
[11].American Cancer Society (Breast Cancer Facts and Figures) 2009-2010.
[12].Fatma M, El-shaken Mahmud F. et al,. Effect of different modalities of treatment on the quality of life of breast cancer patients in Egypt. Eushen Mediterranean Health Journal 1997; 3:68-91.
[13].Perry SH, Kowalski TL, Chang CH. Quality of life in women with breast cancer, Benefits, Acceptability and Utilization. Health Quality Life Outcome, 2007; 12:34-40[Pubmed]
[14]Montazeri A. Health related quality of life of breast cancer patients. A bibliography review of the literature from 1974-2007. Journal of experimental and clinical cancer research, 2008; 1756-9966-27-32[Pubmed]
[15].Welch, I. (2000). Views of financial economists on the equity premium and on professional controversies. The Journal of Business, 73-74: 501-537
[16].Eatmon S. Cancer Overview. Principles and Practices of Radiation Therapy, 2004; 3-20
[17].American Cancer Society (Breast Cancer Facts and Figures), 2003.
[18].Cleary AJ, Thompson PW, Kirwan JR. Quality of life measures British. Journal of Rheumatology, 1996; 35:275-281.[Pubmed]
[19].Maihoff SE. Assessment: Principles and Practices of Radiation Therapy, 2004; 2: 251-253

