Case Report

Nodular Cystic Hidradenoma over the Gluteal Region: A Rare Cytomorphological Diagnosis
* Santosh T, *Hemlata Panwar, *Neeraj Shrivastava,*Vandita Singh,*Nighat Hussain,
- *Department of Pathology &lab Medicine AIIMS, Raipur, Tatibandh, Raipur, Chhatisgarh-12, India
- Submitted: Wednesday, May 10, 2017
- Accepted: Tuesday, August 8, 2017
- Published::Monday, August 14, 2017
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background:
The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology (FNAC) because of its easy accessibility; however the cyto-morphological features of skin adnexal tumours are rarely described in literature.
Case presentation:
A young male presented with solitary subcutaneous nodule over gluteal region measuring 3cm in diameter since 2 years. FNAC was done and showed overcrowded cluster of basaloid to polyhedral cells intermingled with hyaline material and foamy macrophages. Few squamous cells were also seen along with foci of calcification. A cytological diagnosis of adnexal tumour, possibly of eccrine origin was given. The excised nodule was received for histopathological examination and a final diagnosis of Nodular cystic Hidradenoma was made.
Conclusions:
awareness of cytological features by FNAC of skin adnexal tumours is important to prevent misdiagnosis.
Keywords:
Fine-needle aspiration; Nodular hidradenoma; Eccrine; Adnexal tumour.
Introduction
The use of fine needle aspiration (FNA) cytology of cutaneous and subcutaneous nodules for diagnosis of primary epithelial tumours of the skin, cystic lesions, few soft tissue tumours and metastatic tumours has been described in the literature. However, FNA diagnosis of skin adnexal tumours is still limited, due to the scarcity of case reports describing the cytological features of such lesions [1]. The present case report highlights the cytomorphological features of the Nodular cystic hidradenoma. Also known as solid-cystic or clear cell hidradenoma is a benign adnexal tumor that arises from the distal excretory duct of eccrine sweat glands [2]. Mostly seen in adults with a female preponderance of between 4th- 7th decade, and childhood onset has also been documented [3]. Nodular hidradenoma’s are most commonly seen on the scalp, neck, trunk and extremities [2, 3]. It usually presents as slowly enlarging, solitary, freely movable nodule, solid or cystic, measuring on an average 0.5-2 cm in diameter, but can reach 6 cm or more in diameter. Usually, it is covered by intact skin, but sometimes can undergo ulceration with a serous discharge; this feature raises the possibility of malignancy [3]. We hereby discuss the cytological features and the potential diagnostic dilemma that they pose to the cytologist and prevent misdiagnosis for eccrine skin adnexal tumours.
Case Presentation
A young male presented with solitary nodule over the gluteal region since 2 years (Figure 1). Physical examination revealed a well-demarcated reddish nodule of 3 cm in diameter. No ulceration was noted. On palpation, a firm to hard, partially mobile, dermal nodule was noticed. FNAC was done and cytological diagnosis of adnexal tumour possibly of eccrine origin was given.

Figure 1 Photograph showing a solitary, smooth surfaced skin lined nodule of 3.5 cm in diameter over the gluteal region.
The smears revealed overcrowded three-dimensional clusters, sheets and dispersed polyhedral to cuboidal cells intermingled with eosinophilic hyaline material. This extracellular eosinophilic hyaline material was surrounded by few loose cohesive cell clusters, resembling rosette-like structures. Occasional acinar structures formed by cuboidal cells filled with the hyaline material were detected. Cells were polygonal, containing round to ovoid nuclei with bland nuclear chromatin, inconspicuous nucleoli and a moderate amount of eosinophilic cytoplasm. Some cells showed very scanty cytoplasm, imparting a basaloid appearance. Some showed a clear cytoplasm. Few cells of squamoid differentiation were also seen. The specks of calcification, cystic macrophages and bare nuclei were evident in the background (Figure 2). We, therefore, gave the diagnosis as a nodular hidradenoma, eccrine type.
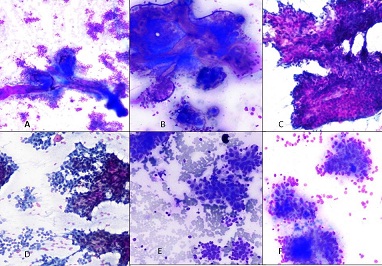

Figure 2 Cytosmears showing (a) three-dimensional clusters intermingled with the hyaline material; (b) polyhedral cells with eosinophilic cytoplasm forming large, cohesive, three-dimensional papillary-like, densely packed clusters; (c) Cells showing ovoid nuclei, bland nuclear chromatin, inconspicuous nucleoli and moderate amount of cytoplasm (d) Papillaroid fronds of polyhedral cells. (e) Cells showing clear cytoplasm; (f) Squamoid cells [Giemsa &PAP, x 40].
Subsequently, a wide excision of the nodule was performed and sent for histopathological examination. On gross, a soft tissue piece measuring 7 x 4.5 x 3.0 cm with overlying skin flap was received. Cut section revealed a well-circumscribed tumour mass measuring 2.5 x 3.0 cm with solid, grey-white homogenous cut surface.
Microscopy revealed a dermal well-circumscribed tumour with sparing of the epidermis. The tumour displayed a nodular, lobulated, cystic and solid growth pattern. The solid area composed of an admixture of both eosinophilic and clear cells separated by bands of hyalinized fibrous tissue. The tumour cells were round to polygonal cells have round to oval nuclei with bland nuclear chromatin and a moderate amount of eosinophilic cytoplasm. Clear cells showed abundant clear cytoplasm with a small, round to oval, eccentric nucleus. Cystic spaces were filled with eosinophilic homogenous material. Foci of calcification and squamous differentiation were also seen (Figure 3). No atypia, invasion, necrosis and mitoses were seen. On the basis of above findings, a histologic diagnosis of nodular cystic hidradenoma was made.
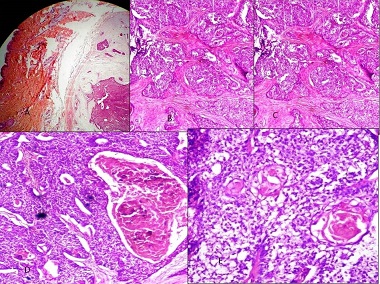

Figure 3 (a) Histopathology showing solid and cystic areas separated by hyalinized band of collagen; solid component composed of polygonal cells with eosinophilic cytoplasm, (Inset) Cells with clear cytoplasm and foci of squamous differentiation seen [H&E x 100].
Discussion
A cytologist may have to face the challenge of diagnosing this skin adnexal tumor as documented in the literature by a few case series and case reports [1-2]. Hence the awareness of the cytological features of adnexal tumors is essential for a cytologist.
The cytological features that characterize the nodular hidradenoma are (i) cellularity is high, (ii) admixture of morphologically different cells like polyhedral cells with central round nuclei and good amount of eosinophilic cytoplasm, cells with clear cytoplasm
squamous looking and basaloid cells, (iii) the cells are seen arranged in three-dimensional clusters, sheets and in a dispersed manner, (iv) rosette-like structures with hyaline material and (v) acinar structures depicting tubular differentiation [3,4]. Our case also had similar features in cytology. Mild hyperchromasia, anisonucleosis and overlapping of nuclei with small distinct nucleoli can also be seen. Eosinophilic cells formed large, cohesive, three-dimensional papillary-like, densely packed clusters. Clear cells form medium-sized, flat clusters. Rounded rosette-like formations and duct-like tubular structures are also seen. The background shows extracellular hyaline amorphous material. Histiocytes, pigmented macrophages, foam cells and naked nuclei may be seen. In the present case similar features were noted [5, 6].
Many authors have proposed that a cytologist may consider a diagnosis of benign eccrine tumour in presence of cohesive clusters of polyhedral to cuboidal cells with cytoplasmic granularity and focal tubule formation [7]. The benign eccrine tumours can be differentiated from malignant lesions by the lack of tight tumor islands with geographic contours and large, atypical cells without any differentiation [5].
Histologically, nodular hidradenoma is a well-circumscribed solid-cystic dermal tumour with a Grenz zone between the tumour and epidermis [8]. Cystic spaces may contain eosinophilic homogenous material. The solid area is composed of an admixture of both eosinophilic and clear cells separated by bands of hyalinized fibrous tissue. Marked nuclear pleomorphism, hyperchromasia or atypical mitoses are not observed [9]. Variants of nodular hidradenoma may show several types of cells [5]. As the quantities of different cell types varies markedly in different tumours, cytopathologists and dermatopathologists should be aware of the resemblance of nodular hidradenoma to other tumors, namely metastatic renal cell carcinoma or squamous cell carcinoma [9].
Conclusion
With this case report, we strive to emphasize the cytological features of eccrine skin adnexal tumour which increase the awareness of the cytologist to prevent misdiagnosis such that effective treatment can be instituted.
Authors’ Contributions
ST
HP
NS:
VS
NH
Competing Interests
The authors declare that there are no competing interests.
Ethical Considerations
The written informed consent was obtained from the patient, a copy of the consent is available with authors.
Funding
None declared
References
[1].Gangne N, Joshi D, Sharma SM. Cytomorphological diagnosis of malignant eccrine tumours: Report of two cases. Diagn Cytopathol 2008;36:801-804. PMID: 18831018 [PubMed]
[2].Nasit JG, Dhruva G. Nodular
hidradenoma of the scalp: A cytomorphological evaluation on fine needle
aspiration cytology. Indian J Dermatol Venereol Leprol. 2014
Nov-Dec;80(6):569-72. [PubMed]
[Free full
Text]
[3].Santosh T, Patro MK, Behera JK, Dash AK. Nodular Hidradenoma: A Rare Cytological Diagnosis. J Cancer Sci Ther 2016; 8:48-49. [Free full Text]
[4].Dubb M, Michelow P. Cytologic features
of hidradenoma in fine needle aspiration biopsies. Acta Cytol 2009;53:179-82. [PubMed]
[5].Agarwal S, Agarwal K, Kathuria P, Jain
M, Chauhan DS, Prakash O. Cytomorphological features of nodular hidradenoma
highlighting eccrine differentiation: A case report. Indian J Pathol Microbiol
2006;49:411-3. [PubMed]
[6].Punia RS, Handa U, Mohan H. Fine
needle aspiration cytology of eccrine acrospiroma. Acta Cytol 2001; 45:1083-5. [PubMed]
[7].Devanand B, Vadiraj P. Fine needle
aspiration cytology of eccrine skin adnexal tumors. J Cytol Histol 2011;2:1-7. [Free
full Text]
[8].Sabag S, Glick T. Fine needle
aspiration of nodular hidradenoma: A case report. Diagn Cytopathol
1996;15:395–397. [PubMed]
[9].Grampurohit VU, Dinesh U, Rao R.
Nodular hidradenoma of male breast: Cytohistological correlation. J Cytol 2011;
28:235-7. [PubMed]
[PMC Full Text]

