Case Report

Soft Tissue Metastsis in Carcinoma Breast: A Case Report
1Seema Khanna, 1Shashi Prakash, 1Satendra Kumar, 1Sanjeev K Gupta
- 1Department of General Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi (U.P.), India.221005
- Submitted: December 23, 2012;
- Accepted: January 23, 2013,
- Published: February 14, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Cancers metastasizing to soft tissue are rare. We here present a case of metastasis from a breast cancer to the soft tissue in back.
Case Report
A 45 years female who was a follow up case previously completed treatment for carcinoma left breast, presented with hard fixed soft tissue mass in lower part of back on right side. FNAC of soft tissue mass showed metastasis from a poorly differentiated adenocarcinoma. Thorough systemic search for the primary tumor was done. CT scan of abdomen revealed contracted gall bladder with stone, gall bladder wall was irregular and thickened with maintained planes all around. Few subcentric periportal lymph nodes present. Open cholecystectomy with wide local excision of the soft tissue mass on the back was done. Post operative histopathology revealed Xanthogranulomatous cholecystitis and deposits from an adenocarcinoma in soft tissue mass.
Discussion
Plaza JA et al (2008) had a series of 118 patients having metastasis to the soft tissue and out of those only 13 cases corresponds to metastasis from breast cancer and 3 of those were having metastasis to the back. However, we have not found any other report of soft tissue mass over back as a metastasis from breast cancer. We strongly suggest histological verification and systemic evaluation, whenever soft tissue masses are located elsewhere even after a curative breast cancer operation.
Conclusion
Soft tissue metastasis from carcinoma breast though uncommon but can present, when it can be confused with a separate soft tissue tumor.
Key word
Breast cancer, soft tissue, metastasis.
Introduction
Cancers metastasizing to soft tissue are rare and can be easily misdiagnosed histologically for a primary soft-tissue sarcoma. Soft tissue is usually not the site of distant dissemination of solid tumors. The clinical distinction between a metastatic neoplasm to soft tissue and a primary soft-tissue sarcoma is critical because treatment and prognosis are markedly different. Metastatic neoplasms to soft tissue can also present as the initial manifestation of an occult primary malignancy. Only few small series and isolated cases of soft tissue metastasis from breast cancer have been reported [1-9]. It has been shown that intramuscular soft tissue metastatic nodules are painful, whereas soft tissue sarcomas scarcely produce pain, but grow slowly [10]. Therefore, painless soft tissue nodules, especially remote from the index tumor are usually regarded as being unrelated to the primary carcinoma. Commonly, some solid tumors, such as lung, kidney, and colon carcinomas, have been known to be a prevalent source of soft tissue metastasis [11] but soft tissue metastasis from a breast cancer is rather a rare entity. We here present a case of metastasis from a breast cancer to the soft tissue in back.
Case Report
A 45 years female presented our surgical outpatients department with pain in right upper part of abdomen for 1 year and a swelling on the lower part of her back on right side for 6 months. (Figure 1) Abdominal examination was unremarkable. 6x4 cm hard, irregular, non-tender mass, fixed to overlying skin was present 4 cm posterosuperior to right posterior superior iliac spine. The patient was a follow-up case of ours treated three and half years back for Carcinoma left breast with modified radical mastectomy and adjuvant chemotherapy. Post operative histopathology was of poorly differentiated infiltrating ductal carcinoma with no tumor deposits in the lymph nodes. The immunohistochemistry showed tumor positive for estrogen and progesterone receptors and negative for HER-2neu.

Figure 1: Soft tissue metastasis from breast cancer.
Ultrasound of abdomen revealed contracted gall bladder with stone and possibility of mass at neck of gall bladder.
CT scan of abdomen revealed contracted gall bladder with stone, gall bladder wall was irregular and thickened with maintained planes all around. Few sub centric per portal lymph nodes present.
FNAC of soft tissue mass showed metastasis from a poorly differentiated adenocarcinoma.
A thorough search was then carried out to detect the primary for this soft tissue metastasis. An X-Ray of the chest, pan-endoscopy and colonoscopy were done; all of them were normal.
With the pre-operative diagnosis of Carcinoma gall bladder with soft tissue metastasis we planned to operate the patient. Intra-operatively we noticed dense adhesions over gall bladder; a contracted, friable gall bladder with grossly thickened and irregular wall with gall stones but without any mass lesion. Gall bladder bed and liver were normal and no significant lymph nodes were noticed. Hence an Open cholecystectomy with wide local excision of soft tissue mass over right side of lower part of back was done. A suction drain was put in the sub-hepatic space.
Post operative course of the patient remained uneventful.
Post operative histopathology of-Gall bladder suggested features of Xanthogranulomatous cholecystitis without any features of malignancy.
Histopathological Examination of the soft tissue mass showed deposits from an adenocarcinoma (Figure 2). To confirm its origin from breast cancer we did receptor study in soft tissue mass which revealed tumor positive for estrogen and progesterone receptors and negative for HER-2neu.
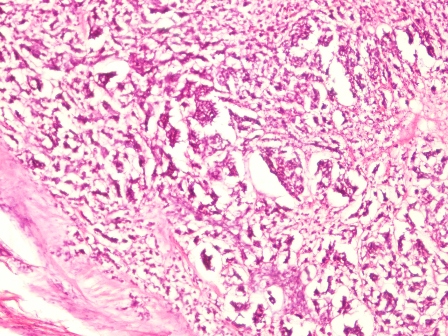
Figure 2: Microphotograph showing metastatic deposits of adenocarcinoma.
Discussion
Despite the finding that soft tissue comprises approximately 55% of our body mass, hematogenous metastases to these areas are rare. Direct extension of a primary tumor to soft tissue is a much more common event than distant soft tissue metastases. Several factors have been implicated in the rarity of this phenomenon such as changes in pH, accumulation of metabolites, and the local temperature at soft tissue sites [5]. Breast cancer is one of the most dreadful cancers for women worldwide. Even though many new chemotherapeutic agents and treatment modalities have led to improved survival of breast carcinoma patients, we often unexpectedly have to face distant dissemination of this ailment. That is the reason why we have to thoroughly examine and follow-up patients utilizing a battery of tests, including radiologic work-up. Breast cancer is known to metastasize to anywhere in the body, either by hematogenous or lymphatogenous routes. Our patient has previously been treated for left breast cancer and now had metastatic soft tissue mass on the right side of the lower part of the back. Abdominal ultrasound and CT scan features were strongly suggestive of a possibility of carcinoma gall bladder and so we had a suspicion for this soft tissue mass being metastasized from gall bladder. With the thorough literature search, we were able to find to find only two large reports on distant soft tissue metastasis [12, 13]. Plaza JA et al., (2008) had a series of 118 patients having metastasis to the soft tissue and out of those only 13 cases corresponds to metastasis from breast cancer and 3 of those were having metastasis to the back [13]. However, we have not found any other report of soft tissue mass over back as a metastasis from breast cancer. Most of the other reported cases indicated skin, kidney, lung, colon, bone, ovary, or cervical cancer as primary tumors, with the clear exception of breast cancer. Hence both painful and painless growing soft tissue masses, irrespective of their distance from the primary breast cancer, should be examined and biopsied to rule out possible metastatic breast cancer. The reason for this is that the prognosis of neglected soft tissue metastases from breast cancer has been death in a span of about five months [12]. It is impossible to precisely determine the route of distant dissemination most of the times. Usually, more than half of the body mass reported resides in soft tissue and blood vessels may not be the route for this type of dissemination [13]. Therefore, usually the origin of the soft tissue mass is from the nearby surroundings. In addition, there may have been so many local or tissue factors identified that make it difficult for cancer cells to travel across the soft tissue [5]. Further, there are no sine qua non features that can confirm this nodule as metastatic breast cancer, except for the fact that it shared histological features with the index breast cancer and no other primary cancer.
Conclusion
Soft tissue metastasis from carcinoma breast though uncommon but can present, when it can be confused easily with a separate soft tissue tumor.
Learning Points
We strongly suggest histological verification and systemic evaluation, whenever soft tissue masses are located elsewhere even after a curative breast cancer operation. In doing so, patients will be saved from dismal prognoses due to improper and delayed diagnosis and treatment.
Authors' Contribution
SP: Planning and execution of treatment, literature search and preparation of the main body of manuscript.
SK: Literature search and involved in the planning and execution of treatment.
SK: Planning and execution of treatment and revision of the manuscript.
SKG: Final decision for the treatment and proof reading of manuscript before submission.
Conflict of Interests
None
References
[1]. Leinung S, Mobius C, Udelnow A, Hauss J, Wurl P. Histopathological outcome of 597 isolated soft tissue tumors suspected of soft tissue sarcoma: a single-center 12-year experience. Eur J Surg Oncol. 2006;33:508–511. [Pubmed].
[2]. Damron TA, Heiner J. Distant soft tissue metastases: a series of 30 new patients and 91 cases from the literature. Ann Surg Oncol. 2000;7:526–534. [Pubmed].
[3]. Tuoheti Y, Okada K, Osanai T, et al. Skeletal muscle metastases of carcinoma: a clinicopathological study of 12 cases. Jpn J Clin Oncol. 2004;34:210–214. [Pubmed].
[4]. Glockner JF, White LM, Sundaram M, McDonald DJ. Unsuspected metastases presenting as solitary soft tissue lesions: a fourteen-year review. Skeletal Radiol. 2000;29: 270–274. [Pubmed].
[5]. Herring CL Jr, Harrelson JM, Scully SP. Metastatic carcinoma to skeletal muscle. A report of 15 patients. Clin Orthop Relat Res. 1998;272–281. [Pubmed].
[6]. Yoshioka H, Itai Y, Niitsu M, et al. Intramuscular metastasis from malignant melanoma: MR findings. Skeletal Radiol. 1999;28:714–716. [Pubmed].
[7]. Viswanathan N, Khanna A. Skeletal muscle metastasis from malignant melanoma. Br J Plast Surg. 2005;58:855–858. [Pubmed].
[8]. Torosian MH, Botet JF, Paglia M. Colon carcinoma metastatic to the thigh—an unusual site of metastasis. Report of a case. Dis Colon Rectum. 1987;30:805–808. [Pubmed].
[9]. Tochigi H, Nakao Y, Horiuchi Y, Toyama Y. Metastatic malignant melanoma in the hand muscle—a case report. Hand Surg. 2000;5:69–72. [Pubmed].
[10]. Sudo A, Ogihara Y, Shiokawa Y, Fujinami S, Sekiguchi S. Intramuscular metastasis of carcinoma. Clin Orthop Relat Res 1993;296: 213-7. [Pubmed].
[11]. Williams JB, Youngberg RA, Bui-Mansfield LT, Pitcher JD. MR imaging of skeletal muscle metastases. AJR Am J Roentgenol 1997; 168:555-7. [Pubmed].
[12]. Damron TA, Heiner J. Distant soft tissue metastases: a series of 30 new patients and 91 cases from the literature. Ann Surg Oncol 2000; 7:526-34. [Pubmed].
[13]. Plaza JA, Perez-Montiel D, Mayerson J, Morrison C, Suster S. Metastases to soft tissue: a review of 118 cases over a 30-year period. Cancer 2008;112:193-203. [Pubmed].

