Case Report

Giant Right Renal Cyst Mimicking Intra-abdominal Malignancy: A Unique Finding
1Soyemi Sunday, 1Faduyile Adedayo, 2Oyewole Olugbenga, 1Sanni Ayodele, 2Popoola Abiodun, 1Obafunwa John, 3Adedeji Modupe, 3Fabanwo Tokunbo
- 1Department of Pathology and Forensic Medicine, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria.
- 2Department of Radiotherapy and Oncology, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria.
- 3Department of Obstetrics and Gynecology, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria.
- Submitted: December 02, 2012
- Accepted: December 18, 2012
- Published: January 12, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Simple cysts are the most common cystic abnormality encountered in the kidney and are caused by large family of hereditary, sporadic, developmental and acquired disorders. Most increase with age and appear to grow more rapidly in younger patients. Association with renal cell carcinoma and hypertension has been reported. Giant renal cyst measuring more than 15.0cm in diameter and containing more than 1500mls of serous fluid are rarely seen.
Case report
We report a case of giant right renal cyst in a 22- year old female of the Yoruba ethnic group in Western part of Nigeria. The cyst measured 60.0 x 42.0 x 25.0cm, with 20,600mls of serous fluid and weighing 12,145gm. She underwent radiological and other routine investigations and subsequently had laparotomy with total excision. Histology confirmed the diagnosis of simple multi-locular renal cyst. The patient had uneventful recovery period and subsequently discharged home after a week in the hospital.
Conclusions
Renal cyst can reach enormous size. This to the best of our knowledge is the largest renal cyst in the medical literature. Studies are needed with particular attention to the factors associated with and if possible the etiology of rapid renal cyst enlargement, the association with hypertension and renal cell carcinoma.
Key words
Giant, cyst, intra-abdominal, renal.
Introduction
Cystic disease of the kidney belongs to a large family of hereditary, sporadic, developmental and acquired disorders .characterised by the presence of cyst in the kidney [1,2]. Simple renal cysts are the most common cystic abnormalities encountered in the kidney [3]. However, it is worth mentioning that multicystic renal dysplasia is the most common form of cystic renal disease in children and the most common cause of abdominal masses in the new born [4]. It has been shown that simple renal cysts are seen in 5-12% of general population undergoing abdominal ultrasound for different reasons [5,6].
They are usually unilocular and can be bilocular or multilocular and usually filled with clear serous fluid and lined by single layer of flattened or cuboidal epitheliun. They occur commonly in the renal cortex, although the aetiology is yet to be fully established, it is believed that they originate from the diverticular of the distal convoluted tubule [7]. Simple cysts increase with age and appear to grow more rapidly in younger patients [6]. Most are asymptomatic with few rarely presenting with abdominal mass, pain, rupture, haemorrhage, haematuria, infection, hypertension or renal obstruction [8,9].

Figure 1: Picture of the renal cyst on the grossing table with a tape measurement.
Giant renal cyst measuring more than 15.0 cm in greatest is rarely seen [10]. However, a giant renal cyst measuring 20.0 cm x 17.0 cm in size and managed by laparoscopic surgery with transperitoneal access [10] was reported.

Figure 2: Gross picture showing prominent vascular channels and areas of hemorrhage.
We report a unique case of a 22- year old female who presented with a massive abdominal distension which was noticed at birth and has increased progressively till presentation. It measures 60.0 cm in greatest diameter at presentation. The uniqueness of this case not only lies with the large size but also with the absence of any signs or symptoms apart from the diffuse, non lateralizing gross abdominal distension.
Case Report
Miss I.S who is a- 22 year old single nulliparous lady with primary school education presented at the gynecology clinic of LASUTH with compliant of abdominal swelling which she noticed from birth.

Figure 3: Gross picture showing prominent vascular channels and brownish-black areas reminiscent of old hemorrhage. There is a solid part on the upper right quadrant of the cystic mass. This is the remaining part of the kidney.
The abdominal swelling was only associated with some discomfort but had no abdominal pain. She also had pressure symptoms like easy satiety, some difficulty in breathing, though had no leg swelling. There was no cough or contact with person with chronic cough. She had no acne, excessive growth (hirsutism), change in voice or baldness of hair. Also, there was no history suggestive of urinary symptoms.

Figure 4: The cystic mass has been opened showing the inner shiny surface.
She attained menarche at 12 years of age with a regular menstrual cycle. Never had she used contraceptives in the past. She had presented at several care centers, disrupting her education. She however presented in our centre for expert management.
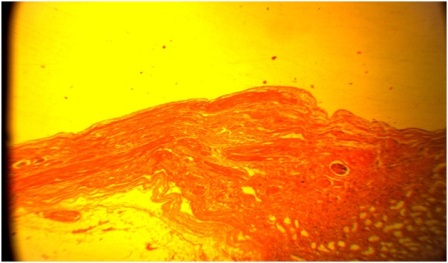
Figure 5: Histological section showing the wall of the cyst lined by flattened epithelium and the wall exhibiting renal glomerulus and tubules. X 40.
At the gynecology clinic, she had an “egg on stick” appearance and otherwise looking healthy. Abdominal examination revealed a grossly uniformly distended non tender abdomen with demonstrable as cites by a positive fluid thrill sign. A normal female external genitalia was noticed.
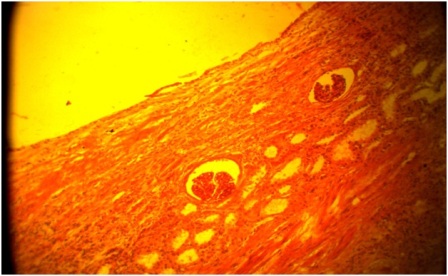
Figure 6: Histological section showing the wall of the cyst lined by flattened to cuboidal epithelium and the wall exhibiting renal glomeruli and tubules with lymphocytic infilterates. X 100.
An impression of abdominal mass with probability of an ovarian tumour was made. Abdomino-pelvic ultrasonography revealed right renal cystic complex mass, CT showed ovarian tumour with markedly thinned- out right kidney while Computerized Tomography and IVU revealed a non visualised right kidney and ureter.
Figure 7: Section of the cyst wall showing the flattened epithelium at higher magnification. X 400.
Exploratory laparotomy was done and findings revealed a huge enucleated cystic mass weighing 22.0 kg, occupying the whole of the peritoneal cavity displacing the bowels into the chest wall and splinting the diaphragm. A normal sized healthy looking left kidney was seen. The uterus and ovaries were visualized which were however looking rather rudimentary. The specimen was thereafter sent for histology. Histology revealed right muitilocular simple renal cyst with chronic pyelonephritis.
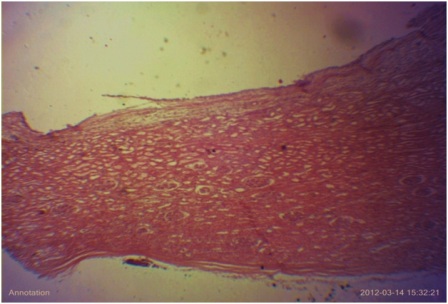
Figure 8: Histological section showing the wall of the cyst lined by flattened epithelium and the wall exhibiting renal glomerulus and tubules. X 40.
Discussion
Renal cyst is one of the most common benign lesions of the kidney and occurring at a frequency greater than 50% in individuals above 50 years and because they are rarely symptomatic, many are found incidentally [11]. Although, coexistence of a renal cyst and renal cell carcinoma has been observed in 0.3% to 2.9%, a tumour arising within a solitary or multiloculated cyst is rare [12].
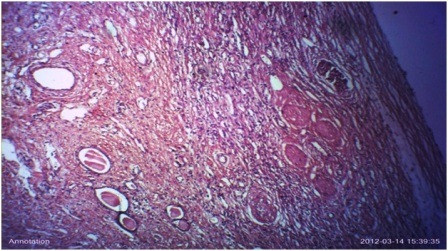
Figure 9: Histological section showing thyroidization of some tubules and lymphocytic infiltrates within the interstitium. This is compatible with chronic pyelonephritis X 100 .
Renal cyst increases with age and a study has shown that the average increase in size and rate of enlargement were 2.82mm and 6.3% yearly. Cyst in patients younger than 50 years grew more rapidly than in patients older than 50 while multiloculated type progressed more rapidly than simple cyst (6.93 versus 2.8mm yearly) [6].
A simple cyst is the most benign lesion of the kidney that may occur well within a kidney or on its surface, usually oval or round in shape, has a smooth outline lined by a single layer of flattened epithelium and filled with a transudate-like clear or straw colored fluid [13]. This is consistent with our gross and microscopic findings. Our mass was oval to round with greyish to light- brown surface and having occasional areas of haemorrhage. The mass weighs 12.5kg and contains 28,000mls of serous fluid with a shinny inner surface. This type of a giant cyst has rarely been reported in any medical literature although brown et al., [4, 10] reported a giant renal cyst measuring 25 cm in greatest diameter presenting with massive abdominal distension. Because of its extremely large size, it may compress and obstruct the urinary tract and produces flank pain or abdominal pain, renal calculi, haematuria and urinary tract infection [14]. It may also lead to hypertension and loss of renal function [14].
Cases of complicated renal cysts have been reported. Most complications are spontaneous rupture, infections and hemorrhage [14]. Hypertension rarely complicates a renal cyst [15]. The association between hypertension and renal cyst has been previously reported. Local renal ischemia caused by renal expansion, leads to stimulation of the renin-angiotensin-aldosterone system and hypertension [15]. Angiotensin II also increases the filtration fraction at the glomerulus and increases sodium reabsorption which leads to tissue hypoxia by increasing the renal oxygen consumption [15, 10]. The association between simple renal cysts and higher arterial blood pressure probably arises from the underlying renal disease causing both. Remission of hypertension after surgical cyst removal has established its relationship with the renal cyst [15, 10].
Most benign renal cysts are asymptomatic and necessitate no treatment [10] however, when symptomatic, flank pain is the most common symptom. A palpable flank mass, haematuria, hypertension, and compression of the pelvicalycael system can also occur [10].
Generally, these lesions do not require treatment but therapy is needed when a renal cyst causes hydronephrosis, pressure atrophy of the renal parenchyma, pain, deteriorating renal function and hypertension [11].
Surgical treatment, although considered a simple procedure, is not free of complications. Percutaneous aspiration and sclerotherapy is associated with low mortality and morbidity than conventional surgery. Aspiration alone is associated with a high recurrence rate. Since the cyst wall epithelium is responsible for active liquid production, it must be destroyed in order to prevent recurrent disease. Few sclerosing agents including Minocycline hydrochloride, Betadine, 50% glucose solution, ethanol and ethanolamine oleate, to mention a few have been used [11].
Other procedural options include laparoscopic excision [10], single-session alcohol sclerotherapy [10], continuous percutaneous catheter drainage with negative pressure [10] and laparoscopic retroperitoneal three trocar technique used for ablation of a giant symptomatic renal cyst [13]. However, the standard management of symptomatic renal cysts in the past was open surgical decortication or nephrectomy. More recently, less invasive therapeutic procedures carried out include retrograde flexible ureterorenoscopy and percutaneous nephroscopy [15].
Successful laparoscopic ablation of asymptomatic giant renal cyst has also been reported [14]. In our case, the patient had total cyst excision and the sample was sent to our department for histopathological examination. We made a diagnosis of simple multiloculated renal cyst with chronic pyelonephritis. Urinary tract infection complicating giant renal cyst has also been reported by Kamal et al., [14]. The patient had uneventful recovery period and subsequently discharged home after a week in the hospital.
A study carried out to evaluate whether continuous percutaneous catheter drainage with negative pressure yielded better results than single-session alcohol sclerotherapy showed that the former is more efficient the latter in the management of giant cysts. For moderately large cysts, the two methods have similar results [16].
Another study done at Baskent University Hospital, Turkey, showed that percutaneous drainage and repeated injection of 95% alcohol appears to be a safe and effective method for sclerosing giant renal cysts [11].
Thus, in conclusion, further studies need to be carried out with particular attention to the factors associated with and if possible the aetiology of rapid cyst enlargement, the association with hypertension and renal cell carcinoma.
Conclusion
Consent was obtained from the department and the patient. This is for the publication of case report and accompanying images.
Authors' Contribution
SSS: is a post-fellowship senior registrar who performed the literature search and prepared the manuscript.
OPP: contributed to the literature search.
OOO, ADS: took the photographs and grossed the specimen.
FFA, SSS: reported the slides.
OJO: is a professor of pathology who reviewed the slides.
AMO: is a senior registrar who assisted during the surgery while.
AOF: performed the surgery.
Conflict of Interests
The authors declare that they have no competing interests.
Ethical Considerations
None
Funding
None
Acknowledgement
We thank the histotechnologist who prepared the slides and assisted during the grossing. We are grateful to the department for given us the approval to report this case.
References
[1]. Bisceglia M, Gallian CA. Senger C, Stallion C, Sessa A. Renal cystic disease : a review. Adv Anat Pathol 2006: 13:26-56. [Pubmed].
[2]. Torres VE, Grantham JJ. Cystic disease of the kidney. In Brenner BM (ed); Brenner's and Rector's the kidney ed. 8, Vol 2, Philadelphia, 2008. WB Saunders, pp 1428 - 1462.
[3]. Nahm AM, Ritz E. The simple renal cyst. Nephrol Dial Transplant. 2000; 15: 1702 - 1704. [Pubmed].
[4]. Joan Rossai. Rossai and Ackeiman's surgical patholgy ed. 10, Vol1, Mosby Elsevier chp 17 pp 1169.
[5]. Murshidi MM, Suwan ZA. Simple renal cyst. Arch Esp Urol 1997; 50: 928 931. [Pubmed].
[6]. Terada N, Ichioka K, Matsuta Y, Okubo K, Yoshimura K, Arai Y. The natural history of simple renal cyst. J Urol 2002; 167: 21 - 23. [Pubmed].
[7]. Baert I, Steg A. Is the diverticulum of the distal and collecting tubules a preliminary stage of the simple cyst in the adult? J Urol 1977; 118 : 707 - 710. [Pubmed].
[8]. Luscher TF, Wanner C, Siegenthaler W, Vetter W. Simple renal cyst and hypertension: cause or coincidence ? Clin Nephrol. 1986; 26: 91. [Pubmed].
[9]. Papanicolaou N, Pfister RC, Yader IC. Spontaneous and traumatic rupture of renal cyst: Diagnosis and outcome. Radiology 1986; 160 : 99-103. [Pubmed].
[10]. Ahallal Y, Khallouk A, Tazi MF, Tazi.E et al. Remission of hypertention after treatment of giant simple renal cyst: a case report. Cases J. 2009 (2): 9152. [Pubmed].
[11]. Bozkurt FB, Boyvat F, Tekin I, Aytekin C. et al. Percutaneous sclerotherapy of a giant benign renal cyst with alcohol. European Journal of Radiology 2001;40:64-67. [Pubmed].
[12]. Ulker V, Ozyurt C, Gursan A. Renal cell carcinoma in a Giant renal cyst: A case report and Review of the literature; International Urology and Nephrology 1996; 28 (2): 141-144. [Pubmed].
[13]. Sandeep S, Vikas K, Harminder P,Dinesh G. A case report: An Unusual Cause of Giant Renal Mass. Journal Indian Academy of Clinical Medicine.2006; 7(3): 252-4
[14]. Hanash KA, Al-Othman K, Mokhtar A, Al-Ghamdi A, Aslam M. Laparoscopic Ablation of Giant Renal cyst. Journal of Endourology.2003;17(9):781-784. [Pubmed].
[15]. Aloui S, Bouraoui S, Salem R et al. Remission of arterial hypertension after the treatment of a giant renal cyst. Saudi Journal of Kidney Diseases and Transplantation.2011;22:151-2. [Pubmed].
[16]. Zerem E, Imamovic G, Omerovic S. Symptomatic simple renal cyst comparison to continuous Negative pressure catheter drainage and single-session alcohol sclerotherapy. Journal of Roentgenology 2008;190(5):1193-1197. [Pubmed].

